Features of the development of fine motor skills in children with dysarthria. The state of motor functions in a child of senior preschool age with dysarthria Psychophysiology of movements and the development of motor functions in ontogenesis
COMMITTEE OF GENERAL AND VOCATIONAL EDUCATION OF THE LENINGRAD REGION
Autonomous educational institution
higher professional education
"LENINGRAD STATE UNIVERSITY named after A.S. PUSHKIN"
Faculty of defectology and social work
department of speech therapy
Course work
"Study of motor development of children of senior preschool age with erased dysarthria"
Specialty: 050715.65 - Speech therapy
Completed by: 4th year student of the correspondence department Levshina Anastasia
Checked by: Candidate of Pedagogical Sciences, Associate Professor E. A. Loginova
Saint Petersburg
Introduction 2
Chapter 1. Theoretical foundations for studying the problem of the motor sphere in preschool children with erased dysarthria
1.1. Psychophysiology of movements and development of motor functions in ontogenesis 6
1.2. Clinical and pedagogical characteristics of children with erased dysarthria 12
1.3. The state of the problem of studying the motor sphere of children with erased dysarthria 19
Chapter 2
2.1. Purpose and objectives of the pilot study 24
2.2. Experimental study of the motor sphere of children of senior preschool age with erased dysarthria 25
Chapter 3. Features of psychomotor functions of children of primary school age with erased dysarthria 39
3.1. The state of general motor skills of children of primary school age with normal speech development and their peers with erased dysarthria 39
3.2. The state of fine motor skills of children of primary school age with normal speech development and their peers with erased dysarthria 44
3.3. The state of articulatory motility of children of primary school age with normal speech development and their peers with erased dysarthria 50
Conclusion 58
Literature 62
Introduction
One of the most important functions of the psyche, which ensures the cognitive activity of the child, as you know, is performed by motor skills. It is a holistic mechanism for the development of the child's psyche, combining emotions, thinking and movements into a single whole, which are conscious and purposeful. The high importance of motor skills determines the need for its training in preschool children, since it is she who carries out the mental regulation of the educational, cognitive and speech activity of the child (M.O. Gurevich M.O., N.I. Ozeretsky, 2009).
The development of a child's motor skills is a complex dialectical process in which the intensive maturation of the motor cortical zones determines the development of the child's psyche as a whole. Thus, the process of formation of voluntary movements in a child occurs by automating motor and orienting-exploratory actions based on the perception of images and words (N.A. Bernshtein, 1966), and the close connection of fine motor skills and speech development determines the speech regulation of movements in a complex extended voluntary activity. (A.R. Luria, 1957). The psychophysiological system that ensures the development of motor skills contributes to the child's adequate response to the environment and the formation of purposeful activities in accordance with this.
The development of the problem of studying the motor sphere in preschool children with erased dysarthria is relevant for the prevention of speech disorders, to identify their individual psychological characteristics.
Studies of the motor skills of children with erased dysarthria show (L.V. Lopatina, 1987 and others) that the pathology of motor functions is expressed in them to varying degrees: from insufficient coordination and mobility of the organs of speech articulation to impaired static and dynamic coordination of arms and legs.
The muscle tone of preschoolers is unstable, the movements are tense and disproportionate. There are violations of the coordination of movements of the arms, legs, fine motor skills of the hands, articulatory motor skills. The most pronounced violations are usually noted in mimic, articulatory and fine motor skills of the hands. Dynamic praxis suffers. Children have difficulty remembering the sequence of movements, with difficulty switching from one series of movements to another. Some preschoolers have difficulty reproducing and retaining the given tempo and rhythm in memory, and do not correct motor errors on their own.
All of the above violations of the motor sphere make it difficult for preschool children with erased dysarthria to adapt to school, and prevent full communication with peers and adults.
This determines the need for a more thorough study of the problem of motor skills in preschool children with erased dysarthria, as one of the most important factors in a child's readiness for school.
aim This work is to study the state and characteristics of the violation of the motor sphere of preschool children with erased dysarthria.
Tasks research:
The study of literature on the research problem.
Determining the content of the methodology of the ascertaining experiment.
Comparative analysis of the obtained data in two groups of subjects.
An object research - the motor sphere of preschool children with erased dysarthria.
Thing research - the level of general, fine and articulatory motor skills in preschoolers with erased dysarthria.
Hypothesis studies - in preschoolers with erased dysarthria, there is an insufficient formation of motor functions, which is more manifested in articulatory and manual motor skills. The severity and nature of underdevelopment of motor skills in children is different, which suggests the need for a differentiated approach in the system of corrective action to overcome obliterated dysarthria in children.
Research methods:
Literature analysis
Selection of research methods
Research base: MBDOU "Kindergarten No. 7 "Crane".
Chapter 1
1.1. Psychophysiology of movements and development of motor functions in ontogenesis
The development of speech regulation of motor functions is the central problem of the physiology and psychology of human voluntary movements. It is only thanks to the word that these movements can acquire that deliberate and conscious character which distinguishes them qualitatively from the so-called voluntary movements of animals.
The doctrine of the motor analyzer is based on the concept of I.P. Pavlov about the dynamic localization of brain functions. According to this concept, the localization of functions implies not fixed centers, but dynamic systems, the elements of which retain their strict differentiation, playing a highly specialized role in the unified activity of the brain.
In the works of A.R. Luria was shown the role of individual areas of the cerebral cortex in the implementation of motor acts. Postcentral, sensitive areas of the cerebral cortex provide kinesthetic, proprioceptive afferentation of a motor act, the correct addressing of motor impulses to the muscle periphery. The lower parietal regions of the cortex, the parieto-occipital regions control the spatial organization of movement. The premotor cortex regulates the temporal serial organization of movements and actions. The frontal regions provide the psycho-regulatory function of a motor act (comparison of a real movement with the original task, verbal regulation of movements).
The structural and functional features of the motor analyzer are that it has extremely rich connections with all the structures of the central nervous system and takes part in their activities, which gives reason to talk about its special significance in the development of the activity of the entire brain.
Research N.A. Bershtein showed that a motor act is determined by a motor task that is formed at different levels of motor regulation. Since a person makes movements that differ in the degree of arbitrariness, in participation in the motor act of speech, then the degree of control of these movements will be different. ON THE. Bernstein developed the theory of level organization of movements. It allows you to decompose a complex motor act into its constituent components and reveal the state of cerebral levels, their role in the regulation of movements and actions.
In his works, N.A. Bernstein described how movements are controlled. He singled out the cerebral levels of building movements, giving them conditional names according to the first letters of the Latin alphabet, taking into account the morphophysiological characteristics of the level. Each level of movement construction is characterized by morphophysiological localization, leading afferentation, specific properties of movements, the main and background role in motor acts of higher levels, pathological syndromes and dysfunction.
N.A. Bernshtein developed a theory of level organization of movements, including subcortical and cortical levels.
Motor development proceeds in close connection with psychomotor. The development of the concept of "psychomotor" is associated with the name of I.M. Sechenov. He was the first to note the most important role of muscle movement in the knowledge of the surrounding world. This also changed the idea that existed before about the executive function of the motor centers of the cortex, called psychomotor. Research by I.P. Sechenov played a decisive role in understanding psychomotor as the objectification in muscle movements of all forms of mental reflection; in the understanding of the motor apparatus, which performs an epistemological and praxeological function as an integrator of all human analyzer systems.
Motor control, carried out at the early stages of ontogeny exclusively by direct signaling, later on begins to be carried out with the continuously increasing participation of the verbal system. It appears both in the form of verbal instructions and demands of the surrounding people, and in the form of the intentions of the child himself, formulated with the help of external or internal speech. The significance of speech in the transformation of motor functions from involuntary, unconscious to arbitrary, consciously regulated has long been noted in the scientific literature. So, the outstanding domestic anatomist and teacher, the founder of the modern system of physical education P.F. Lesgaft back in the 80s. XIX century persistently pointed out the role of the word in the formation of the child's ability to consciously control their movements.
Research M.M. Koltsov and others made it possible to reveal some features of the development of the mechanism of the second signaling system and to understand the main stages of this process in ontogeny.
Researchers pointed to the connection between speech and motor and speech analyzers, the connection between pronunciation and the nature of movements. There is a correlation between the degree of development of fine motor skills of the hand and the level of development of speech in children "... there is every reason to consider the hand as an organ of speech - the same as the articulatory apparatus, from this point of view, the projection of the hand, there is another speech area of the brain" .
All human activity in the process of motor education is dependent on higher nervous activity and is determined both by the anatomical maturation of the central nervous substrates, their myelination, and by the functional maturation and adjustment of the work of coordination levels.
The natural ontogenesis of motor skills in general and fine motor skills in particular consists of two phases that are sharply different in time.
The first phase is the anatomical maturation of the central nervous substrates, which is delayed by the time of birth and ends by 2-2.5 years in relation to the myelination of the pathways.
The second phase, which sometimes passes far beyond the age of puberty, is the phase of functional maturation and the adjustment of the work of coordination levels. In this phase, the development of motor skills is not always directly progressive: at some moments and in relation to certain classes of movements (i.e., levels), temporary stops and even regressions can occur, creating complex fluctuations in proportions and balance between coordination levels.
In the first six months of a child's life, the mechanism of innervation of antagonist muscles gradually improves: on the 1st-2nd month, asynchronous, disordered activity of antagonist muscles is observed, and on the 5th-8th month their synchronous activity appears, but without signs of economical regulation.
Children are born with a number of ready-made motor reflexes that provide them with adaptation to their new habitat: the “breast search” reflex, the sucking reflex, the stepping reflex, the grasping reflex, the tonic neck reflex, the Moro reflex.
By 4 months, some of these unconditioned reflexes disappear (such as the stepping reflex) or become conditioned reflexes.
In the first 3 months of life, the child performs active involuntary (so-called massive) movements. At the 6th month, the tone and coordination of the activity of the antagonist muscles become favorable for the implementation of voluntary movements.
At 4 months, a certain meaningfulness begins to appear in the infant's behavior, indicating the onset of a new stage in the development of psychomotor skills - the appearance of voluntary movements.
At about 4 months of age, babies can successfully reach for objects, although these attempts are still quite clumsy. But it is especially important that at the age of 4-5 months the child's hand begins to play the role of a manipulator organ. Visual-motor coordination develops, i.e., the implementation of motor actions under the control of vision.
All this becomes possible only with a certain level of regulation of visual function, which during the first months of a child's life develops independently of motor function. Well-defined, controlled by the occipital oculomotor center, automatic visual tracking of the object manifests itself from the 2nd month of life. At the age of 4-6 months, voluntary control of eye movements develops, which is associated with the functioning of the frontal oculomotor center. Arbitrary tracking, which ensures the receipt of spatial visual information by children of this age, is carried out by spasmodic eye movements (saccades) and only in the 2nd year of life does it turn into smooth tracking. At the age of 5-6 months, a single visual-motor system is formed, which provides the ability to control arbitrary movements in space.
The first elementary manipulations with objects are inaccurate and are accompanied by synkinesis. At the 5th month, the child can take the object with both hands. At the age of 4 to 6 months, voluntary regulation of eye movement also develops. This ensures the formation of a single oculomotor system in 5-6 months. At the age of 7-10 months, visual-motor coordination reaches a high development: the child can already open and close the lid of the box, put the ball into a hollow cube, and take out one object that attracted his attention with the help of another. However, games with objects in children under 10 months old are still purely manipulative in nature: objects are shifted from hand to hand, they are thrown, they are knocked, etc.
Starting from 10-12 months, a new qualitative leap begins in the psychomotor development of the child.
Firstly, by this time, the physiological basis of walking has already been sufficiently formed - the automatic stepping reflex, as well as the ability to maintain body balance, as a result of which the child begins to walk independently and without support.
Secondly, his games with objects acquire a functional character: the doll is rocked, the comb is “combed”, the car is rolled.
At the age of 12 months, fine motor skills become even more perfect - the child can take small objects and examine them, holding them between the thumb and forefinger.
However, it should be borne in mind that the individual variation in the timing of children mastering certain movements, judging by the literature data, is quite high and can even be several months.
At 18 months, children can build a tower of two to four cubes, eat on their own and hold a spoon.
At the age of 2-3 years, the fine motor skills of children are already quite highly developed. They learn to throw the ball with both hands, pour water from one container to another, draw scribbles, undress on their own.
At preschool age, children can draw with a pencil simple shapes and figures, draw with paints, build constructions from cubes. They can dress and undress independently, if the clothes are simple enough, serve themselves at the table. They learn to catch the ball, which indicates the development of their hand-eye coordination (manual dexterity and the ability to extrapolate).
At this age appears new stage in the development of hand-eye coordination. At the age of 5, 30-50% of children already effectively use the mechanism of preliminary visual afferentation, which can be associated with an increase in the role of proprioceptive afferentation in the control of voluntary movements, which exercises current control over movements, and a decrease in the role of reverse visual afferentation. The latter remains the leading role only in the programming of movements.
At 5-6 years old, fine motor skills improve, so children can fasten and unfasten clothes, some learn to tie shoelaces.
In previous years, it was assumed that the stages in the motor development of children reflect the process of maturation of the motor system. Currently, the entire motor development of the child is considered according to the theory of dynamic systems: motor development involves many individual skills that are organized and reorganized over time to meet the requirements of specific tasks.
Dysarthria is a severe and complex violation of the sound side of speech. Dysarthria (from the Greek. dys - a prefix meaning disorder, arthroo - articulately pronounce) - a violation of pronunciation due to insufficient innervation of the speech apparatus with lesions of the posterior frontal and subcortical regions of the brain.
Dysarthria speech is usually understood as speech that is unclear, blurry, deaf, often with a nasal tinge. To characterize it, the expression is used - "as if porridge in the mouth." Dysarthria occurs as a result of damage to the nervous executive apparatus of speech with one or another localization of the lesion in the central nervous system.
For the first time, the clinical picture of dysarthria was described more than a hundred years ago (A. Oppenheim, H. Gutzman and others). A mild degree of dysarthria as a speech disorder that differs in its pathogenesis was isolated from the group of sound-producing disorders by A. Kussmaul in 1888. Calling tongue-tied all the shortcomings of speech, A. Kussmaul, along with functional, singled out organic tongue-tied tongue, which, in his opinion, was one of the forms of a central, organically conditioned speech disorder. A. Kussmaul for the first time revealed those factors that entail dysarthria speech disorders, manifested in the form of pronunciation ambiguity of varying severity.
An analysis of the literature data showed that there are various definitions of dysarthria.
Dysarthria is a disorder of the pronunciation side of speech, in which the prosodic side of the sound stream suffers, the phonetic coloring of sounds or the incorrect implementation of phonemic signal signs of the sound structure of speech (omissions, substitutions of sounds). This definition of dysarthria is given in the textbook L.S. Volkova and V.I. Seliverstov.
Dysarthria is a violation of the coordination of the speech process, which is a symptom of damage to the motor analyzer and efferent system. At the same time, the ability to segment speech and articulation as a whole is impaired. (K. Becker, M. Sovak).
Both definitions are important, since the first is based on the external manifestations of the pathology, while the second more indicates the presence of dysarthria as a symptom of damage to the central and peripheral nervous system. Thus, the following definition of dysarthria has been identified in modern literature.
Dysarthria is a violation of sound pronunciation and the prosodic side, due to organic insufficiency of the innervation of the muscles of the speech apparatus. This definition reveals, first of all, the symptoms of this disorder and its mechanism.
Etiology:
Dysarthria is a symptom of a complex cerebral lesion of a bulbar, pseudobulbar and cerebellar nature. The etiology of cerebral palsy and dysarthria as a symptom of cerebral palsy is not well understood. Previously, it was believed that the main reason is birth injury. But as studies of recent years (E.N. Vinarskaya) have shown, more than 80% of cases of this pathology are congenital disorders of the brain, that is, intrauterine disorders. Based on these studies, it can be said that the pathology that occurs during childbirth is a secondary cause, which in turn can aggravate the effect of the primary one.
Specific causes leading to brain damage can operate in different periods: prenatal (basic), natal and postnatal.
In the prenatal period, toxicosis, maternal diseases in the first half of pregnancy, chronic maternal diseases: cardiovascular diseases, pulmonary tuberculosis, severe gastrointestinal diseases and liver diseases, diseases of the urogenital area, alcoholism are noted.
The natal period is characterized by pathology of childbirth (dry protracted or rapid delivery), asphyxia of the newborn, group - and Rhesus - conflict situation.
In early postnatal development, the following features are distinguished: motor restlessness, inexplicable sleep disturbance, difficulty holding the nipple, lethargy of the act of sucking, followed by rapid fatigue, frequent choking, profuse regurgitation, breast rejection is possible. There is an inability to keep the head in a vertical position up to 5-7 months, a delay in the process of walking (up to 1 year 2 months).
The diseases suffered by the child during that period also have a great influence: viral influenza, pneumonia, severe forms of gastrointestinal diseases, often colds and infectious diseases, in some cases accompanied by convulsive seizures against the background of high temperature.
In short, we can identify some specific causes leading to brain damage and the occurrence of dysarthria in the prenatal (basic), natal and postnatal periods.
- 1) Prenatal period, that is, prenatal. The most common causes of intrauterine brain damage are: maternal diseases during pregnancy (viral, infectious); the mother has cardiovascular and renal failure; mental and physical trauma during pregnancy; increased dose of radioactivity during pregnancy; influence of nicotine, alcohol and drugs; mismatch between mother and fetus in terms of the Rh factor and group affiliation. The influence of these causes is especially dangerous in the first trimester of pregnancy.
- 2) Natal period (secondary aggravating factors): traumatic brain injury during childbirth; hemorrhage in the brain as a result of a sharp change in pressure (with rapid childbirth, with caesarean section); unsuccessful use of obstetrics (primary cause).
- 3) Postnatal period: diseases transferred by the child himself (meningitis, meningo-encephalitis and others); traumatic brain injury. It is important to note that prenatal distress often entails distress in the natal and postnatal periods.
It should be noted that children with dysarthria according to clinical and psychological characteristics can be conditionally divided into several groups depending on their general psychophysical development: dysarthria in children with normal psychophysical development; dysarthria in children with cerebral palsy; dysarthria in children with oligophrenia; dysarthria in children with hydrocephalus; dysarthria in children with mental retardation; dysarthria in children with MMD (minimal brain dysfunction).
In the symptoms of dysarthria, speech and non-speech symptoms are distinguished.
Non-speech include: massive violations of the motor apparatus or motor sphere; violation of the emotional-volitional sphere; violation mental development; violation cognitive activity; peculiar formation of personality; violation of articulation, breathing, muscle tone. Movement disorders usually manifest themselves for more than later dates the formation of motor functions, especially such as the development of the ability to sit down independently, crawl with alternate simultaneous extension of the arm and the opposite leg and with a slight turn of the head and eyes towards the extended arm, walk, grab objects with the fingertips and manipulate them.
Emotional-volitional disorders are manifested in the form of increased emotional excitability and exhaustion of the nervous system. In the first year of life, such children are restless, cry a lot, require constant attention. They have sleep disturbances, appetite, predisposition to regurgitation and vomiting, diathesis, gastrointestinal disorders. Such children, as a rule, are weather dependent.
At preschool and school age, they are motorally restless, prone to irritability, mood swings, fussiness, often show rudeness, disobedience. Motor restlessness increases with fatigue, some children are prone to reactions of the hysteroid type.
Despite the fact that children do not have pronounced paralysis and paresis, their motor skills are characterized by general awkwardness, lack of coordination, they are awkward in self-service skills, they lag behind their peers in dexterity and accuracy of movements, they have a delay in developing hand readiness for writing, therefore, for a long time no interest in drawing or other activities manual activity, at school age, poor handwriting is noted. Disorders of intellectual activity are expressed in the form of low mental performance, memory and attention disorders.
Many children are characterized by a slow formation of spatio-temporal representations, optical-spatial gnosis, phonemic analysis, and constructive praxis.
Speech symptoms include: violation of sound pronunciation; violation of the prosodic side of speech; violation of phonemic functions. Fuzzy, slurred speech does not allow the formation of a clear auditory image of the word, which in turn further exacerbates sound pronunciation defects; violation of the lexical and grammatical structure of speech; reading and writing impairment.
Thus, dysarthria are the most common speech disorders in children. Clinical features and severity of disorders depends primarily on the location and severity of brain damage.
Send your good work in the knowledge base is simple. Use the form below
Students, graduate students, young scientists who use the knowledge base in their studies and work will be very grateful to you.
Posted on http://www.allbest.ru
FEDERAL AGENCY FOR EDUCATION
STATE EDUCATIONAL INSTITUTION OF HIGHER PROFESSIONAL EDUCATION
"URAL STATE PEDAGOGICAL UNIVERSITY"
INSTITUTE OF SPECIAL EDUCATION
DEPARTMENT OF PSYCHOPATHOLOGY AND LOGOPEDICS
Formation of the motor sphere in the system of correction of phonetic and phonemic underdevelopment of speech in children with mild pseudobulbar dysarthria
Course work
specialty 050715 "Speech therapy"
performed by a third-year student,
302 groups of correspondence department
Luchnikova Ludmila Olegovna
scientific adviser
A.V. Kostyuk
Yekaterinburg - 2013
Introduction
CHAPTER 1. The current state of the problem of studying and the formation of the motor sphere in children with dysarthria
1.1 Definition of the main concepts of the topic
1.2 Ontogeny of the development of motor function in normal children
1.3 Relationship of speech development with the development of motor functions
1.4 Clinical, psychological and pedagogical characteristics of children with mild pseudobulbar dysarthria
Conclusions for chapter 1
CHAPTER 2. Violation of the motor sphere in children with dysarthria
2.1 Organization and methodology for studying the motor sphere and the phonetic side in children with dysarthria
2.2 Features of the development of the motor sphere in children with dysarthria
2.3 Violation of the phonetic side in children with dysarthria
2.4 Mechanism of motor impairment in children with pseudobulbar dysarthria
CHAPTER 3. Logopedic work on the formation of the motor sphere in preschool children with dysarthria
3.1 Rationale and principles speech therapy work on the formation of the motor sphere in children with dysarthria
3.2.1 Formation of the motor basis of movement
3.2.2 Formation of the kinesthetic basis of movement
3.2.3 Formation of the kinetic basis of movement
Literature
INTRODUCTION
During the first years of a child's life, his brain does a huge amount of work in terms of complexity and volume. At this time, the child gets acquainted with the objective world around him, masters speech, learns to communicate with people. It would hardly be an exaggeration to say that a very important role in mastering speech belongs to the motor analyzer.
In childhood, the connection between the body and the psyche is very close. All the experiences of the baby are immediately reflected in his well-being, appearance. Moreover, mind and body develop inseparably from each other. The movement, at first, very simple, and then more and more complex, gives the child the opportunity to explore the world, communicate with others, and, therefore, learn and comprehend.
But at the same time, any developmental disorder in childhood also affects the motor sphere. Movement as a complex, multi-layered system is, as it were, a “mirror” of the state of the child, on the one hand, and a “window” through which we can influence his development, on the other hand.
The motor system affects the entire organism as a whole, but the influence of proprioceptive afferentation on brain activity is especially great. Both the forms and the ways of this influence are very diverse.
THEM. Sechenov was the first to point out the fact that all stimuli are of a mixed nature: an irritant that is adequate for the eye, ear, skin, etc. is necessarily mixed with a “muscular feeling”.
One can watch without listening, or listen without looking; one can smell without hearing or seeing, but one cannot look, listen, smell, or touch without moving. pseudobulbar dysarthria motor speech therapy
Speech arises in the presence of certain biological prerequisites, and above all, the normal maturation and functioning of the central nervous system. Speech is, first of all, the result of the coordinated activity of many areas of the brain. Articulatory organs only carry out orders coming from the brain. MM. Koltsova in the book "The child learns to speak" emphasizes the importance of developing fine motor skills of the hands for the development of the child's speech. The development of fine motor skills of the hands is of great importance for the overall physical and mental development of the child throughout preschool childhood. It is the small muscles of the hands, like the higher parts of the brain, that provide the work of thought and the function of speech.
Speech disorders in children are diverse in their manifestations. A common speech disorder among preschool children is pseudobulbar dysarthria, which tends to increase significantly. Dysarthria is based on organic disorders of the central nervous system. In children, clumsiness of motor skills is noted, which is most clearly manifested when performing complex motor acts that require precise control of movements, the precise work of various muscle groups, and the correct spatio-temporal organization of movements. Both articulatory and general motor skills of the child are disturbed. In this regard, articulatory positions are created in a distorted, approximate form.
In the cerebral cortex, the speech area is located next to the motor area, so the work on the formation and improvement of voluntary motor skills is considered as a necessary component of a complex system of correctional and pedagogical impact. The more attention is paid to this issue, the more effectively and quickly a positive result will be achieved.
Therefore, the aim of the work is to correct the oral speech of preschoolers with the help of games and exercises aimed at developing arbitrary motor skills (general, fine motor skills of fingers, facial expressions and articulation).
Hypothesis: timely diagnosis of fine motor disorders will allow you to properly build work to overcome phonetic and phonemic underdevelopment of speech in preschoolers with mild pseudobulbar dysarthria.
Based on the purpose of the work, tasks follow.
To study and analyze the accumulated experience in the study of general, fine and articulatory motor skills in the scientific and methodological literature
Conduct a survey of general, fine and articulatory motor skills and correlate the level of underdevelopment of the motor sphere with defects in sound pronunciation
Determine the direction of corrective work.
Object: the formation of motor functions in children with phonetic and phonemic underdevelopment of speech, a mild degree of pseudobulbar dysarthria.
Subject: the formation of fine motor skills as the basis for the development of speech in children with a mild degree of pseudobulbar dysarthria.
CHAPTER 1
1.1 Obasic definitionvtopical concepts
Speech is a complex functional system, which is based on the use of the sign system of the language in the process of communication. The most complex system of language is the product of a long socio-historical development and is assimilated by a child in a relatively short time.
The speech functional system is based on the activity of many cerebral structures of the brain, each of which performs a specific operation of speech activity.
The structural-systemic organization of the integration of brain functions involves a multilevel interaction of vertically organized (subcortical-cortical) and horizontal (intercortical) systems. Despite the fact that each functional system has its own program of development and functioning, the brain in all periods of life works as a whole. This integrativity is determined by the close interaction and interconnections both between sections of the cerebral cortex (horizontal systems) and the interconnections of the cortex with the underlying brain formations and, above all, the subcortical parts of the brain (vertical systems). The connection of speech activity with brain structures is based on the modern ideas of A.R. Luria. Dynamic localization of brain functions implies a holistic and at the same time differentiated involvement of the brain in any of the forms of its activity. [Volkova]
Various parts of the cerebral cortex are involved in the implementation of speech. These departments include, first of all, the cortical speech zones located in the dominant hemisphere. These are auditory, motor and visual areas. In the temporal lobe of the left hemisphere, perception and differentiation of auditory stimuli take place, and a complex process of speech understanding is carried out in it; the motor area (lower frontal gyrus of the left hemisphere) carries out the program of speech utterance, i.e. actually motor speech; in the visual area (occipital lobe) there is a perception and recognition of graphic images necessary for written speech.
A necessary condition for the organization of voluntary movement (motor speech) is the apparatus of the frontal lobes of the brain. With the help of these devices, the creation, preservation, implementation of the program of action and constant control over its course are carried out.
The second condition for performing a voluntary movement is the preservation of its kinesthetic afferentation. Kinesthetic sensations are sensations of the position of parts of one's own body and the muscular efforts produced during and outside of movement. This type of sensation occurs as a result of irritation of special receptor formations (proprioreceptors) located in muscles, tendons, joints and ligaments. They provide information about the movement and position of the body in space.
The role of kinesthetic sensations in mental activity was highlighted by I.M. Sechenov, who believed that the muscular sense is not only a regulator of movement, but also the psychophysiological basis of spatial vision, time perception, objective judgments and conclusions, abstract verbal thinking.
Kinesthetic sensations are closely related to the work of receptors located on the surface of the body and perceiving stimuli from the external environment: taste, pain, temperature, visual. This is especially pronounced in the sense of touch, which is a combination of kinesthetic and skin sensations, in which important role visual, auditory, vestibular analyzers, etc. play. Muscular-motor sensitivity also contributes to the correct orientation in space.
Underdevelopment of kinesthetic sensitivity causes an increase in motor insufficiency when performing particularly complex movements, which require movement control, precise dosing of muscle efforts, accuracy, spatio-temporal organization of movements, that is, sensorimotor coordination.
The cortical apparatuses of kinesthetic analysis and synthesis are the postcentral parts of the brain. With underdevelopment or damage to the lower parts of the post-central region of the cortex of the left hemisphere, kinesthetic apraxia occurs. In these cases, there are no paralysis, paresis, muscle strength is sufficient. The kinesthetic afferentation of the motor act suffers, the movements become undifferentiated. Violation of the organization of movements of the speech apparatus, facial muscles is manifested in the inability to find the positions of the lips and tongue necessary to pronounce the desired sounds.
The third condition for successful voluntary movement is fast and smooth switching from one motor position to another. The cortical apparatuses of kinesthetic analysis are the lower sections of the premotor region of the left dominant hemisphere. Underdevelopment or damage to the premotor areas of the cerebral cortex is manifested in the inertia of motor stereotypes, in motor perseverations of the hand, articulatory apparatus, and in speech.
The fourth condition for the organization of voluntary movement is the preservation of the parieto-occipital regions of the cerebral cortex. With the help of these devices, visual-spatial afferentation of movement is carried out. [Z.A. Repina]
Auditory, visual, motor and kinesthetic analyzers take part in the implementation of the speech function. The extrapyramidal system also takes part in the implementation of the motor mechanisms of speech. The strio-pallidar system is involved in the preparation of a motor and speech act and its correction in the process of execution, regulates the tone of the speech muscles, and provides emotional expressiveness of speech; The cerebellum is involved in coordinating the rhythm, rate of speech, and tone of the speech muscles.
Thus, for normal speech activity, the coordinated functioning of the entire brain is necessary. With the defeat of various parts of the nervous system, a variety of speech disorders can occur; the nature of these disorders depends on the location and time of the lesion.
Sound speech is carried out due to the influence of three physiological functions: respiration, voice formation, articulation. These functions originate in certain organs of our body: lungs, diaphragm, larynx with vocal folds, and articulatory apparatus. Active organs of articulation take part in the formation of sounds: lips, tongue, lower jaw, soft palate; vocal apparatus: larynx with vocal folds and pharynx; fixed organs of articulation: hard palate, teeth, upper jaw.
All organs involved in speech are innervated by twelve pairs of cranial nerves. The motor centers in the cerebral cortex are connected to the nuclei in the brain stem regions by corticonuclear pathways. The speech act is reflex in nature. Speech reflexes are associated with the activity of the entire cerebral cortex and constitute the second signaling system.
All movements of the lips and tongue are determined by the work of the motor analyzer. Its function is the perception, analysis and synthesis of stimuli that go to the cortex from the movements of the organs of speech. In the motor speech zone, a complex and subtle differentiation of speech movements occurs, the organization of their sequence. [Arkhipova]
Currently, the most common speech disease among preschool children is pseudobulbar dysarthria. At the heart of speech disorders in pseudobulbar dysarthria are organic lesions of the pathways of the cranial nerves.
All forms of dysarthria are characterized by disorders of general and articulatory motility, characterized mainly by insufficiently fine coordination of speech muscles and insufficient manipulative finger activity. This is due to the fact that speech, being a part of general motor skills, is formed on the basis of the combined maturation of the speech-motor functional system. The main signs of dysarthria are defects in sound pronunciation and voice, combined with speech disorders, primarily articulatory motility and speech breathing. Depending on the type of impairment, all defects in sound pronunciation in dysarthria are divided into anthropophonic (sound distortion) and phonological (lack of sound, replacement, undifferentiated pronunciation, mixing).
For all forms of dysarthria, articulatory motility disorders are characteristic, which manifest themselves in a number of ways. Violations of muscle tone, the nature of which depends primarily on the localization of brain damage. The following forms are distinguished in the articulatory muscles: spasticity of the articulatory muscles - a constant increase in tone in the muscles of the tongue, lips, in the facial and cervical muscles. With a pronounced increase in muscle tone, the tongue is tense, pulled back, its back is curved, raised up, the tip of the tongue is not expressed. The tense back of the tongue, raised to the hard palate, helps soften consonant sounds. Therefore, a feature of articulation with spasticity of the muscles of the tongue is palatalization (this is a softening of consonants resulting from the raising of the middle back of the tongue to the hard palate.), which can contribute to phonemic underdevelopment.
A decrease in muscle tone speaks of dysarthria of the paretic type. At the same time, the tongue is thin, flattened in the oral cavity, the lips are flaccid, there is no possibility of their complete closure. Because of this, the mouth is usually half open, hypersalivation is pronounced. Feature of articulation - nasalization.
Violations of muscle tone in the articulatory muscles with dysarthria can also manifest themselves in the form of dystonia (changing the nature of muscle tone): at rest, there is a low muscle tone in the articulatory apparatus, when trying to speak, it increases sharply.
1.2 Ontogeny of the development of motor functions in children is normal
The development of motor functions in the ontogenesis of a child occurs very slowly - over many months and years. All movements first appear as innate, and only in the course of the development of the child do they acquire a conditioned reflex character, i.e. are brought into connection with stimuli with which they were previously associated, or new combinations of several movements are developed. From the first days of life, the child has an innate grasping reflex, which by the end of the 1st month becomes weaker and gradually fades away; at the age of about 4 months, the child begins to reach for a bright object and grasps it - now the same grasping movement is the result of learning, i.e. acquires a conditioned reflex character. At the age of 8-9 months, the child has a further complication of the grasping reflex: he captures a large object with his entire palm and fingers, and a small one - only with his fingers, i.e. movements of various muscles are combined depending on the size of the object to be grasped.
It is interesting that both simple movements and some complexly coordinated motor acts are innate, this includes not only many complex innate nutritional and defensive reactions (sucking, swallowing, sneezing, etc.) - locomotions of walking, swimming in the early stages child development are found to be congenital. In the first weeks of life, a swaddled baby makes stepping movements, and if you put him in water on his tummy, then swimming. Around the age of three months, the innate walking and swimming movements "disappear", and as developed, they can only be obtained at an older age. Congenital include quite complex facial reactions of children, also based on coordinated movements of several muscle groups: from the first days of life, babies give adequate facial reactions to various taste stimuli, at the age of 2 to 6 months they have a pronounced imitation of the facial expressions of adults. At the 7th month, the unconditioned reflex imitation of facial expressions fades away, and as a developed reaction, it is noted in children only at the age of about two years.
Among other motor functions, the movement of the fingers of the hand is of particular importance, because. have a huge impact on the development of the higher nervous activity of the child. V.M. Bekhterev wrote that hand movements have always been closely connected with speech and contributed to its development.
The first motor function of the hand is grasping. Like other motor acts, grasping is first revealed as an innate reflex (the Robinson grasping reflex). At 4-5 months, the grasping of an object acquires a developed, i.e. conditioned reflex, character and is performed with the imposition of all fingers and palms on the object - the so-called "monkey grasping". Only at the 9th month the child begins to take the object with his fingers, and at the 11-12th month the first attempts to use the objects for their intended purpose appear: drink from a cup, scoop up porridge with a spoon, comb hair, etc. [M.M. Koltsova].
In the development of each neuropsychiatric function, critical periods arise when it becomes, as it were, a priority, the most significant for the brain. For the development of such a function, it is necessary to quickly mobilize the reserves of the body, at the expense of already previously formed functional systems, which are less protected, less compensated. In this regard, the most important feature of critical periods of development is not only the development of a priority function, but also, as a rule, some decompensation of other functions.
In each age period, it is necessary to determine not only the priority developing function, but also “weak spots” - those functions whose development rate is temporarily reduced, which reveal a temporary insufficiency of their compensation and are the most vulnerable to adverse environmental influences.
Differentiation of psychoneurological functions begins in early childhood. First, basic functions are distinguished and developed, primarily perception, then more complex ones. Perception, intensively developing, as if moves forward to the center of consciousness and becomes the dominant mental process. Moreover, the perception itself is not sufficiently differentiated, it is merged with emotions. The remaining functions remain on the periphery of consciousness, they depend on the dominant function. The period when the function dominates is the period of its most intensive, optimal development. Perception dominates in early childhood, memory dominates in preschool, and thinking dominates in primary school.
The motor function can be conditionally divided into two relatively independent functions, which have their own developmental features:
1. Gross motor skills, i.e. motor skills of the trunk and limbs, which includes the processes of verticalization, balance, support and walking;
2. Fine motor skills of the hands.
The newborn has chaotic impulsive movements of the limbs, which gradually become more free and purposeful. In the first 3 months of life, the development of motor skills is manifested mainly in line with the "revitalization complex". By 2 months, the child masters the ability to raise and hold his head. From about 2-3 months, the development of hand movements begins in the direction of a visible object, then grabbing and holding it. From this time on, the child begins to feel objects.
By about 5-6 months, hand movements are improved: the child can accurately direct his hand to an object, take it. Based on these movements, subject-manipulative activity develops. At the age of 3 to 7 months, the child masters the movements, on the basis of which rollover is mastered, and then crawling. From the 8th month, the child gradually learns to sit, sit and lie down, as well as get up, stand and lower himself, holding on to the support with his hands. By one year, the child walks independently.
At early preschool age, the coordination of hand movements is improved, in connection with which the independence of the child is significantly increased: he learns to dress, undress, wash, etc., subject activity becomes more complicated. The child can throw the ball at the target, catch it. Walking, climbing are improved, the child learns to run, jump, perform simple rhythmic and dance movements to the music. At preschool age, various sports skills become possible: cycling, swimming, skiing, skating. Becomes available visual activity: modeling, drawing, application.
At 4 years old, a child can balance on one leg for up to 5 seconds, jump 20 centimeters in length and jump on two legs and one right leg.
By the age of five, a child has the elements of a step that are characteristic of an adult, which is due to the improvement of the mechanisms for controlling the functions of walking - the distribution of muscle loads, the pace of movements, and speed. Further formation of dominance allows a child of this age to jump separately on the right and left legs. Fine motor skills of the hand develop and, at the same time, step automatism is finally dissociated, the functions of the hand are “liberated” from the influence of the legs. By the age of five, a child can simultaneously perform two types of movements - running and throwing a ball.
Speech development
Speech development goes through three stages. I period - preverbal - falls on the first year of life and includes the stages of cooing, babbling. In the course of preverbal communication with others, the prerequisites for speech development are formed. The condition for mastering speech is the formation of selective susceptibility to the speech of others - the preferential selection of it among other sounds, as well as a finer differentiation of speech influences compared to other sounds. There is a sensitivity to the phonemic characteristics of sounding speech. The preverbal stage of development ends with the child's mastering the understanding of the simplest statements of an adult, the emergence of passive speech.
II period - the transition of the child to active speech. It usually occurs in the second year of life. The child begins to pronounce the first words and simple phrases, phonemic hearing develops. Of great importance for the timely acquisition of speech by a child and for the normal pace of its development at the first and second stages are the conditions of communication with adults: emotional contact between an adult and a child, cooperation between them and saturation of communication with speech elements.
III period - improvement of speech as the leading means of communication. It more and more accurately reflects the intentions of the speaker, more accurately conveys the content and general context of the reflected events. There is an expansion of the dictionary, the complication of grammatical structures, the pronunciation becomes clearer. But the lexical and grammatical richness of speech in children depends on the conditions of their communication with other people. They learn from audible speech only what is necessary and sufficient for the communicative tasks facing them. [Skvortsov]
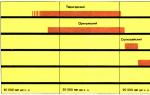
Table compiled on the basis of the results of studies conducted at the STC PNI.
|
The development of general motor skills and speech of a child from birth to 5 years is normal |
|||||
|
Child's age |
Gross motor skills |
fine motor skills |
Impressive speech |
expressive speech |
|
|
All unconditioned reflexes are evoked, symmetrical |
Fingers clenched into a fist, single, rare "athetoid" finger movements |
||||
|
Tries to tear his head off the surface on which he lies, but cannot hold it, drops it and turns to the side Tries to lift head while lying on stomach |
|||||
|
1,5 months |
Raises the head by 45 degrees, lying on the stomach, holds it for 10-20 seconds, while the legs are tense |
||||
|
In the position on the stomach, they hold the head, while the arms under the chest are bent at the elbow joints, actively moves the legs Holds head upright (for a short time) |
Opens the cam |
Spontaneously pronounces individual sounds, reflectively hums |
|||
|
Lying down, can lean on forearms (several minutes) |
Holds the toy put into the brush, pulls it into the mouth |
||||
|
Raises arms above horizontal level more often |
Sometimes grasps an object with the hand |
||||
|
Foot support appears |
Reaches for a toy, grabs it |
Active cooing |
|||
|
Actively raises head from supine position Flips over to the side |
Grabs the toy with two fingers, brings it to the mouth, throws it |
||||
|
Sits with support, keeping head steady |
Begins to grab small objects |
In response to speech addressed to the child, a response vocal activity occurs. |
Actively spontaneously melodious hums with chains of sounds |
||
|
Strong foothold when standing with support |
Shifts a toy from hand to hand |
Babble is manifested by short sounds (vowels in combination with labial consonants) |
|||
|
Lying on his stomach, the child can extend one arm Sitting in a passive posture |
Responds to his own name |
Active undifferentiated babble |
|||
|
Rolls over from back to stomach |
Various active babbling (anterior-lingual, posterior-lingual, etc.), autoecholalia |
||||
|
Rolls from belly to back Crawling without engaging the pelvic girdle |
Actively manipulates objects |
Understands verbal commands with gesture reinforcement |
|||
|
Synchronized crawling Independently squats from a prone position, through the side |
Begins to select parts of the face of a doll and an adult by word |
Double sound combinations like "ba-ba" appear |
|||
|
Protective extension of the arms forward and to the sides, allowing you to maintain balance Stands in a pose on his knees |
Uses thumb to grip Knocks with a toy on a toy |
Visually differentiates named familiar objects |
|||
|
Sits down independently from any positions and sits confidently |
Starts purposefully manipulating a pyramid of 2-3 rings (removes, discards) |
Understands verbal commands without gesture reinforcement |
|||
|
Moves on his knees on his own |
Tries to put dice on dice |
On request, finds familiar objects located in an unusual place |
Imitating an adult, learns new syllables |
||
|
Stands at a support, gets up on his own |
Picks up small objects with index and thumb |
Shows confidently parts of the face of a doll and an adult Begins to recognize objects in one-object pictures |
Calls people and objects syllables |
||
|
Worth it on its own Walks with support |
Tries to string rings on the pyramid rod |
At the direction of an adult, performs actions with toys Understands the word "no" |
|||
|
Walks alone |
Can flip the pages of a cardboard book Lowers small objects into a narrow opening |
Executes many commands as requested |
Speaks about 5 words (mother, grandmother, grandfather, etc.) |
||
|
Walks for a long time, turns |
Turns 2-3 pages at the same time |
Shows multiple body parts |
Associates syllables with a specific subject Expresses desires through speech (appearance of verbs) |
||
|
Steps over obstacles |
Draws doodles, strokes tearing paper |
Shows all parts of the body |
Speaks about 10 words (mostly titles) |
||
|
Tries to run Goes up and down the stairs with side steps, holding on to the railing |
Turns one page at a time |
Shows all objects in everyday life |
Two word sentences |
||
|
Stands up and squats independently Bends over and picks up objects from the floor |
Hand preference is formed Repeats vertical and round lines as shown |
Shows a lot of pictures |
Makes sentences of 3-4 words |
||
|
Standing on one leg without support Climbs, descends stairs, alternating legs (with support) Can ride a tricycle |
holding a pencil correctly |
Can answer a question based on a story in one word Executes about 10 instructions consisting of one action |
Asks questions with the words “who?”, “Where?”, “Where?” (word order is not always correct) Easily repeats phrases |
||
|
Jumping on two legs |
Copies a circle Unbuttons buttons |
Tries to use plural, past tense Uses negative particles "not", "neither" 3.6 uses adjectives and pronouns Asks questions "when?", "what's inside?", "why?" Able to communicate with an adult Uses complex sentences |
|||
|
Able to roll forward Jumping on one leg |
Copies a square (fuzzy, with folded corners) Cutting paper with scissors |
Can answer abstract questions, eg. "does the sun shine at night" |
Uses polite requests Uses future tense Uses the definition of space: "on", "under", "behind" |
||
|
Performs two types of movements at the same time |
Copies triangle Correctly draws a square |
There is an understanding of the abstract concepts of "friendship", "truth", "deception", etc. |
There is a combination of simple sentences into complex ones. The emergence of divisive questions Can describe his feelings Begins to use the abstract concepts of "happiness", "love", "hope", "lie" |
1.3 The relationship of speech development with the development of motor functions
All scientists who have studied the activity of the child's brain, the psyche of children, note the great stimulating effect of the functions of the hand.
An outstanding Russian educator of the 18th century N.I. As early as 1782, Novikov argued that "the natural impulse to act on things" in children is the main means not only for gaining knowledge about these things, but for everything from mental development.
Neurologist and psychiatrist V.M. Bekhterev wrote that hand movements have always been closely connected with speech and contributed to its development.
The English psychologist D. Selly also attached great importance to the "creative work of the hands" for the development of thinking and speech in children.
The movements of the fingers of people improved from generation to generation, as people performed more and more subtle and complex work with their hands. In this regard, there was an increase in the area of the motor projection of the hand in the human brain. So, the development of the functions of the hand and speech in people went in parallel.
Physiologists attached great importance to the muscular sensations that arise during articulation. The development of sound pronunciation is associated with the improvement of the work of the peripheral speech apparatus. In healthy children, mastery of the sound system of the language occurs simultaneously with the development of motor and differentiated hand movements.
The motor speech area is located very close to the motor area, and the area of the motor projection is occupied by the projection of the hand, located very close to the speech motor area. The magnitude of the projection of the hand and its proximity to the motor speech zone led many scientists to the idea that the training of the fingers will have a great influence on the development of the child's active speech.
The movements of the fingers historically, in the course of the development of mankind, turned out to be closely related to the speech function. First, the child develops subtle movements of the fingers, then the articulation of syllables appears, all subsequent improvement of speech reactions is directly dependent on the degree of training of the movements of the fingers.
The articulation of sounds, the so-called "motor speech", consists in the coordination of movements of the tongue, lips, oral cavity, larynx, and respiratory movements. The motor projection of the organs of speech is located in the lower part of the anterior central gyrus, while the process of coordination of movements is carried out in Broca's motor speech area, located in the lower part of the frontal gyrus. In the motor projection of various parts of the body in the precentral gyrus, more than 1/3 of the area is occupied by the projection of the hand. In addition, the projection of hand movements and speech zones are located in close proximity. It was the size of the projection of the hand and its proximity to the motor speech zone that led scientists to the idea that the training of fine movements of the fingers should have a greater impact on the development of active speech in children than the training of general motor skills.
Throughout early childhood this dependence clearly stands out - as the fine movements of the fingers improve, the speech function develops. Of particular importance is the period when the opposition of the thumb to others begins - from that time on, the movements of the remaining fingers become freer.
Research by scientists from the Institute of Physiology of Children and Adolescents of the APN (M.M. Koltsova, E.I. Isenina, L.V. Antakova-Fomina and others) confirmed and substantiated the relationship between speech and finger motor skills. In an electrophysiological study conducted by T.P. Khrizman and M.I. Zvonareva, it was found that when a child makes rhythmic movements with his fingers, the coordinated activity of the frontal and temporal parts of the brain sharply increases in him. If the child produces rhythmic movements (extension and flexion) with fingers right hand, then in the left hemisphere of the brain, he has an increase in coordinated electrical oscillations precisely in the frontal and temporal zones. The movements of the fingers of the left hand caused the same activation in the right hemisphere.
L.A. Panashchenko, children in the first weeks of life were observed in the orphanage. Biocurrents of the brain were recorded in six-week-old babies, then the right hand was trained in some of these children, and the left in others. The training consisted of massaging the hand and passive flexion and extension of the fingers. A month and two months after the start of such training, the biocurrents of the brain were re-recorded and the degree of stability in the appearance of high-frequency waves was calculated by mathematical methods (which is an indicator of the maturation of the cerebral cortex). It turned out that after a month of training, high-frequency rhythms began to be observed in the area of motor projections, and after two months - in the future speech zone, in the hemisphere opposite to the trained arm!
The described data of electrophysiological studies directly indicate that the speech areas are formed under the influence of impulses coming from the fingers. [Koltsova]
1.4 Clinical, psychological and pedagogical characteristics of children with a mild degree of pseudobulbar dihartria
In children with a mild degree of pseudobulbar dysarthria, pronounced paralysis and paresis are not observed, but their motor skills are characterized by general awkwardness, lack of coordination, they are helpless in self-service skills, lag behind their peers in dexterity and accuracy of movements, their hand readiness for writing develops with a delay, therefore for a long time there is no interest in drawing and other types of manual activities.
Emotional-volitional disorders are manifested in the form of increased emotional excitability and exhaustion of the nervous system. In the first year of life, such children are restless, cry a lot, require constant attention. They have sleep disturbances, appetite, predisposition to regurgitation and vomiting, diathesis, gastrointestinal disorders. They do not adapt well to changing weather conditions.
At preschool and school age, children with dysarthria are restless, prone to irritability, mood swings, fussiness, often show rudeness, disobedience. Motor restlessness increases with fatigue. Others are shy, inhibited in a new environment, adapt poorly to it, and avoid difficulties. [L.S. Volkov]
Ogeneral motor skills.
Children with erased dysarthria are motor awkward, the range of active movements is limited, the muscles quickly get tired during functional loads. They stand unsteadily on one leg with one leg, cannot jump on one leg, walk along the “bridge”. They do not imitate well when imitating movements: how a soldier walks, how a bird flies, how bread is cut, etc. Motor failure is especially noticeable in physical culture and music lessons, where children lag behind in pace, rhythm of movements, as well as when switching movements.
Mfine motor skills.
Children learn self-service skills late and with difficulty: they cannot fasten buttons, untie a scarf, etc. in drawing classes, they do not hold a pencil well, their hands are tense. A lot of people don't like to draw. Particularly noticeable motor awkwardness of the hands in the classroom for applications and with plasticine. In the works on the application, there are also difficulties in the spatial arrangement of elements. Violation of fine differentiated hand movements is manifested when performing finger gymnastics tests. Children find it difficult or simply cannot perform imitation movements without outside help, for example: “lock”, “rings” and other finger gymnastics exercises. In origami classes, they experience great difficulties and cannot perform the simplest movements, because. both spatial orientation and subtle differentiated hand movements are required. Many children under 5-6 years old are not interested in games with the designer, they do not know how to play with small toys, they do not collect puzzles.
Features of the articulatory apparatus
In children with pseudobulbar dysarthria, pathological features in the articulation apparatus are revealed. It is possible to decrease, increase or change the nature (dystonia) of muscle tone.
With reduced muscle tone, muscle paresis is said. Pareticity of the organs of articulation is manifested in the following: the face is hypomimic, the muscles of the face are flaccid on palpation, because the lower jaw is not fixed in an elevated state due to the lethargy of the masticatory muscles; lips are flaccid, their corners are lowered; during speech, the lips remain sluggish and the necessary labialization of sounds is not produced, which worsens the prosodic side of speech.
The tongue with paretic symptoms is thin at the bottom of the oral cavity, sluggish, the tip of the tongue is not very active. With functional loads (articulation exercises), muscle weakness increases.
With increased muscle tone, speaking of spastic symptoms. Spasticity of the muscles of the organs of articulation is manifested in the following: the face is amimic, the muscles of the face are hard and tense on palpation. The lips of such a child are constantly in a half-smile: the upper lip is pressed against the gums, during speech, the lips do not take part in the articulation of sounds. Many children who have similar symptoms cannot perform the tube exercise. The tongue is tense, raised up in a hillock, to the hard palate.
Features of sound pronunciation
In her works, E.F. Arkhipova writes that a child with a mild degree of pseudobulbar dysarthria reveals: mixing, distortion of sounds, replacement, and absence of sounds. In addition to impaired sound pronunciation, the prosodic side of speech is also impaired in children. All this affects speech intelligibility, intelligibility and expressiveness of speech.
Phonetic and prosodic disorders in erased dysarthria are due to paresis or spasticity of individual muscles of the articulatory, vocal and respiratory sections of the speech apparatus. The variability and mosaic nature of these disorders cause a variety of phonetic and prosodic disorders:
interdental pronunciation of the anterior lingual in combination with the throat [r];
lateral pronunciation of whistling, hissing and affricates;
softening defect: due to the spasticity of the tip of the tongue and the tendency to its more anterior articulation;
Whistling sigmatisms: are formed when hissing due to the paresis of the tip of the tongue are formed in the lower position of the tongue;
hissing sigmatisms: can be explained by spasticity of the tongue, when the tongue is thickened and tense;
voicing defects: they should be considered as a partial voice disorder, phonation disorders and other phonetic disorders [Arkhipova]
In many studies devoted to the study of the problem of the erased form of dysarthria, it is noted that in children of this category, violations of phonemic perception are common. [V.A. Kisileva].
Phonetic - phonemic underdevelopment of speech
Phonetic and phonemic underdevelopment is a violation of the processes of formation of the pronunciation system of the native language in children with various speech disorders due to defects in the perception and pronunciation of phonemes.
R.E. Levin and V.K. Orfinskaya, on the basis of a psychological study of children's speech, came to the conclusion that phonemic perception is essential for the full assimilation of the sound side of speech. It was found that in children with a combination of impaired pronunciation and perception of phonemes, there is an incompleteness of the processes of formation of articulation and perception of sounds that differ in subtle acoustic and articulatory features. The state of phonemic development of children affects the mastery of sound analysis.
Secondary underdevelopment of phonemic perception is also observed in violations of speech kinesthesia that occur with anatomical and motor defects of the speech organs. In these cases, the normal auditory-pronunciation interaction, which is one of the most important mechanisms for the development of pronunciation, is disrupted. The low cognitive activity of the child during the period of speech formation, weakened voluntary attention, is also important.
With a primary violation of phonemic perception, the prerequisites for mastering sound analysis and the level of formation of sound analysis skills are lower than with a secondary one.
The most common form of disturbance is distorted pronunciation of sounds, in which some similarity of sound with the normative sound is preserved. Usually, in this case, the perception of hearing and differentiation with close sounds does not suffer.
This form of impairment, such as the absence of sound or replacement by articulation close ones, creates conditions for the mixing of the corresponding phonemes and complications in acquiring literacy.
When mixing close sounds, the child develops articulations, but the process of phoneme formation is not yet completed. In such cases, it is difficult to distinguish between close sounds from several phonetic groups, and the corresponding letters are mixed.
In the phonetic-phonemic development of children, several conditions are revealed:
Insufficient discrimination and difficulty in analyzing only sounds that are disturbed in pronunciation. The rest of the sound composition of the word and the syllabic structure are analyzed correctly. This is the easiest degree of phonetic - phonemic underdevelopment;
lack of distinction a large number sounds from several phonetic groups with their well-formed articulation in oral speech. In these cases, sound analysis is violated more severely;
With deep phonemic underdevelopment, the child “does not hear” the sounds in the word, does not distinguish between the relationship between sound elements, is not able to distinguish them from the composition of the word and determine the sequence.
The low level of proper phonemic perception is most clearly expressed in the following:
fuzzy distinction by ear of phonemes in one's own and someone else's speech (primarily deaf - voiced, whistling - hissing, hard - soft, etc.);
· unpreparedness for elementary forms of sound analysis and synthesis;
difficulty in analyzing the sound composition of speech. [Volkova]
Conclusionsonfirstchapter:
1. An analysis of the literature has shown that for normal speech activity, the coordinated functioning of the entire brain is necessary. Great importance in the development of speech function.
2. Pseudobulbar dysarthria is a common disease among preschool children.
3. It is noted in the literature that in children with dysarthria there are violations of articulatory, general, fine motor skills. Children with pseudobulbar dysarthria have a late development of motor functions.
CHAPTER 2MOTOR DISORDERS IN CHILDREN WITH DYSARTRIA
2.1 Organization and methodology for the study of the motor sphere and phoneticeside in children with dysarthria
Examination of children was carried out on the basis of general education kindergarten No. 49 in Polevskoy. Speech therapy examination was carried out with children of the senior group of the general education kindergarten. The group consists of 5 children 5-6 years old.
Logopedic examination was carried out using guidelines edited by Trubnikova, as well as the examination methodology proposed by V.A. Kisileva. Recommendations for conducting a speech therapy examination are based on a general systematic approach, which is based on the idea of speech as a complex functional system, the structural components of which are in close interaction. A comprehensive comprehensive examination of the features of the development of speech, mental functions, the motor sphere, the activity of various analyzer systems will allow us to give an objective assessment of the existing shortcomings in speech development and outline the best ways to correct them.
At the preparatory stage, medical documentation was studied, a conversation was held with parents and educators.
At the next stage, a survey of general, fine, articulatory motility and mimic muscles was carried out. The state of sound pronunciation, phonemic hearing, vocabulary and grammar was studied. All proposed tests are performed by showing, then by verbal instructions. The recommendations propose a rating system, taking into account the nature, severity and number of errors made. The scores are determined on the basis of a scale: 4 points - high level, 3 points - average, 2 points - below average, 1 point - low level
A general motor test was carried out:
Static coordination of movements
Samples were also conducted to examine fine motor skills:
kinesthetic praxis
· Dynamic praxis
Investigation of motor coordination
When examining articulatory motility, the child was offered the following tasks:
Maintaining a static posture
Tasks for the examination of kinesthetic praxis
Dynamic coordination of movements
Examination of mimic muscles
Examination of the pronunciation of sounds
Examination of the syllabic structure
Phonemic hearing test
2.2 Features of the development of the motor sphere in children with dysarthria
E.F. Arkhipova, studying the anamnestic data of children early age, notes a delay in locomotor functions: motor awkwardness when walking, increased exhaustion when performing certain movements, inability to jump, step over stairs, grab and hold the ball.
There is a late appearance of the finger grip of small objects, a long-term preservation of the tendency to capture small objects with the whole brush. In the anamnesis, there are difficulties in mastering self-care skills, dislike for drawing; many children do not know how to hold a pencil correctly for a long time.
L.V. Lopatina notes that in children with an erased form of dysarthria, both statics and dynamics of movements are disturbed. Among the movements that reflect the state of static coordination, the most difficult to perform are voluntary movements, which manifests itself either in some stiffness of movements, the impossibility of performing more complex movements, or in motor restlessness, in the presence of hyperkinesis, in the difficulty or impossibility of finding and maintaining a given position, in the presence of synkinesis. Among the movements that reflect the state of dynamic coordination, tasks associated with switching movements are difficult to perform. Switching movements is often difficult, with a long search for the desired position, incomplete, slow pace, with the appearance of accompanying movements, with a violation of lightness and smoothness. Even more difficult is the possibility of simultaneous execution of movements. [Lopatina L.V.] In the study of the motor skills of children with pseudobulbar dysarthria, Lopatina, tests proposed by N.I. Ozeretsky, E.Ya. Bondarevsky, M.V. Silver.
A test for static coordination of movements shows that static disorders are manifested in significant difficulty (and sometimes impossibility) of maintaining balance, in tremor of the limbs. When holding a pose, children often sway, trying to maintain balance, lower their raised leg, touching the floor with it, and rise on their toes.
Test for dynamic coordination of movements. Performing a dynamic test shows that in more than a third of cases, children throw the ball at the target not from the extended shoulder, but from below. At the same time, at the moment of throwing with one hand, the other is tense and brought to the body. The performance of tasks for the study of dynamic coordination of movements is characterized by insufficiently coordinated activity of various muscle groups, "jerky", clumsiness of the movements performed.
Test for the study of the speed of movements. The performance of the task to study the speed of movement shows that more than half of the children find it difficult to sit on the floor and stand up without the help of their hands. Basically, the task is performed in slow motion. Children are able to sit on the floor without the help of hands, but cannot rise without this help. They rely on either one or both hands. The nature of the children's performance of the task confirms the insufficient formation of dynamic coordination of movements and motor maneuverability, which was found when performing other tests.
...Similar Documents
Stages of formation of sound pronunciation in children are normal. Clinical-psychological-pedagogical characteristics of children with dysarthria; examination of their motor sphere, pronunciation skills and phonemic hearing. Planning of corrective work with preschoolers.
term paper, added 11/24/2012
Psychological and pedagogical characteristics of children with motor alalia. Principles, methods of corrective action. Experimental study of children with motor alalia. Methodology for the study of the level of speech underdevelopment. Ascertaining experiment, its analysis.
term paper, added 02/02/2011
Reasons for violation of the letter. Clinical, psychological and pedagogical characteristics of children of primary school age with pseudobulbar dysarthria, directions of corrective speech therapy work to eliminate the shortcomings of written speech in this category of children.
thesis, added 04/19/2014
Dysarthria as a complex speech disorder. Approaches of various researchers to the definition of the essence of pseudobulbar dysarthria. Patterns of mastering speech by a child. Development of a correctional and developmental program for the correction of pseudobulbar dysarthria.
term paper, added 06/05/2012
Stages of formation of oral speech and motor sphere in children are normal. Psychological and pedagogical characteristics of children with dysarthria. Development of a set of exercises aimed at the development of motor functions in the structure of overcoming the general underdevelopment of speech.
thesis, added 03/29/2012
Features of the speech development of children with dysarthria in cerebral palsy, distinguishing them from children with normal speech development. Speech therapy experimental training of preschool children with dysarthria in cerebral palsy on the formation of the pronunciation side of speech.
thesis, added 04/08/2011
Review of the problem of the development of the phonetic-phonemic side of speech in the psychological and pedagogical literature. The work of a speech therapist on the development of the phonetic-phonemic side of speech in preschoolers with erased dysarthria, the development of a set of games to correct the defect.
thesis, added 03/11/2012
Psychological characteristics of children with a mild degree of mental retardation, the specifics and problems of the communicative sphere. The study of the level of school anxiety in adolescents with mild mental retardation and adolescents with intact intelligence.
thesis, added 06/23/2013
Diagnosis of features of speech development in preschool children with erased dysarthria. Methodological approaches to the construction of speech therapy work on the correction of phonetic and phonemic disorders in children of this category in the process of didactic play.
thesis, added 03/18/2011
Clinical-psychological-pedagogical characteristics of children with dysarthria. A review of existing methods for examining phonetic and phonemic perception in children of primary preschool age with dysarthria. Quantitative manifestation of defects in the pronunciation of sounds.
There is a close functional connection between the speech function - its motor, executive component - and the general motor system. Normal human speech is provided by the coordinated work of many brain structures.
With dysarthria in children, mimic, articulation disorders are noted in combination with a violation of fine and general motor skills.
Diagnosis and complex correction of motor functions in dysarthria in children, providing for medical and psychological-pedagogical measures, is an urgent but little studied problem.
Download:
Preview:
MDOU d / s No. 38 of the combined type of the Molochny settlement of the Kola district of the Murmansk region
Overcoming motor disorders in older preschool children with dysarthria.
caregiver
highest qualification category
Markova R.B.
Murmansk
2011
There is a close functional connection between the speech function - its motor, executive component - and the general motor system. Normal human speech is provided by the coordinated work of many brain structures.
With dysarthria in children, mimic, articulation disorders are noted in combination with a violation of fine and general motor skills.
Diagnosis and complex correction of motor functions in dysarthria in children, providing for medical and psychological-pedagogical measures, is an urgent but little studied problem.
In the first half of the 19th century, an important discovery was made, which played a decisive role in the ideas about the mechanisms of motion control. A significant step forward was the work of I.M. Sechenov "Reflexes of the brain", which substantiated the reflex nature of voluntary human movements and deeply revealed the role of muscle sensitivity in controlling movements in space and time, its connection with visual and auditory sensations.
The mechanism of purposeful action is a complex functional system. The most important processes inherent in it are: the inclusion of motor automatisms; synthesis of afferent signals for the formation of a motor task and the creation of an action program; kinesthetic control and the formation of new motor automatisms.
He clearly outlined the idea that the voluntary movements of a person are inherently psychomotor, since they are certainly associated with such a mental phenomenon as a motive. This means that first the idea of the need for movement appears, and only then - the movement itself.
The connection of movements with the psyche is not limited to this. The psyche not only determines movement, but also manifests itself in motor reactions. Psychomotor is the objectification of all forms of mental reflection in sensorimotor, ideomotor and emotional-motor reactions and acts.
Thus, the psychomotor (or motor) sphere of a person consists of two large blocks: motor skills and motor qualities (abilities).
Some authors, for example, V.A. Kiseleva and A. Semenovich emphasize that speech motor skills include two aspects - facial and articulatory motor skills. In the works of L.V. Lopatina and N.V. Serebryakova and others, the term "articulatory motility" is used as a synonym for the term "speech motility". Within the framework of this approach, the following definition can be cited.
Under the articulatory motility of L.S. Volkova implies "a set of coordinated movements of the organs of the speech apparatus and providing one of the conditions for correct sound pronunciation." The pronunciation of speech sounds is a complex motor skill that a child masters from infancy, making a lot of various articulatory and facial movements with the tongue, lips, lower jaw, accompanied by diffuse sounds (cooing, babbling). They are the first stage in the speech development of the child. The accuracy, strength and differentiation of these movements develop in the baby gradually. One of the conditions for the correct formation of sound pronunciation is the sufficient development of speech motor skills. To correctly pronounce the sounds of speech, the child must be able to reproduce the necessary articulatory structures, including a complex set of movements.
Thus, when pronouncing various sounds, the mobile speech organs (tongue, lips, lower jaw) occupy a strictly defined position.
In works devoted to the issues of motor skills and speech, the connection of speechand expressive movements (A.A. Leontiev), the relationship between motor and speech analyzers (A.R. Luria), the relationship of pronunciation features with the nature of articulatory movements (G.V. Chirkina, N.V. Nishcheva).
EAT. Mastyukova attached great importance to the fact that speech is closely connected ontogenetically, anatomically and functionally with the motor system. Emphasizing that speech is the most vulnerable to the effects of various harmful factors on the central nervous system, she found in children with cerebral pathology, at all stages of their age development, a relationship between the dynamics of the development of motor speech.
Ontogenetic features of the development of motor skills in the sphere are described in the studies of G.N. Kryzhanovsky, E.M. Mastyukova, V.I. Seliverstova et al. These authors note that a child is born with very little control over his own body. A little later, he will learn to control it under the influence of gravity, gradually stabilize it and control its movements. Children are born with a number of ready-made motor reflexes "search for the breast", sucking, walking, grasping, neck-tonic, etc.), which provide them with adaptation to their new environment. By 4 months, some of these unconditioned reflexes disappear (such as the walking reflex) or become conditioned reflexes. In the first 3 months of life, the child performs active involuntary movements. At the 6th month, the tone and coordination of the activity of the antagonist muscles become favorable for the implementation of voluntary movements. At 4 months, the baby can roll over from his stomach to his back and vice versa. Approximately at this age, a certain meaningfulness begins to appear in the infant's behavior, indicating the onset of a new stage in the development of psychomotor skills - the appearance of voluntary movements.
At about 4 months of age, babies can successfully reach for objects, although these attempts are still quite clumsy. But it is especially important that at the age of 4-5 months, the child's hand begins to play the role of a manipulator organ. Visual-motor coordination develops, i.e. implementation of motor actions under visual control. All this becomes possible only with a certain level of regulation of the visual function, which during the first months of a child's life develops independently of the motor function. At the age of 5-6 months, a single visual-motor system is formed, which provides the ability to control arbitrary movements in space. At the 5th month, the child can take the object with both hands. At the age of 4 to 6 months, voluntary regulation of eye movement also develops. This ensures the formation of a single oculomotor system in 5-6 months. At the age of 7-10 months, visual-motor coordination reaches a high development: the child can already open and close the lid of the box, put the ball into a hollow cube, and take out one object that attracted his attention with the help of another.
Starting from 10-12 months, a new qualitative leap begins in the psychomotor development of the child. Firstly, by this time, the physiological basis of walking has already been sufficiently formed - an automatic stepping reflex, as well as the ability to maintain body balance, as a result of which the child begins to walk independently and without support. Secondly, his games with objects acquire a functional character: the doll is rocked, the car is rolled.
During early childhood, visual-motor coordination continues to improve. By age 2, most children can climb stairs, walk backwards, and kick a ball. Children after 2 years of age begin to develop control in a new aspect. The left and right side become controlled by two opposite parts of the brain: the left side - the right side of the brain, and the right side - the left side of the brain. Organizing movements around this midline is vital to learning various physical actions. Somewhere from 18 months to 6 years, these skills develop. Many of these centers stabilize the torso and train both arms, which is essential for complex tasks such as eating with a spoon, opening a door, buttoning, pouring, writing. This process is called developing a preference for using the hand. For most people, this is the right hand, the left hand takes on an accompanying role.
At the age of 2-3 years, the psychomotor skills of children are already quite highly developed. They learn to run, jump on two legs, kick the ball with their feet, throw the ball with both hands, draw scribbles, undress themselves.
At the age of 3, when walking and running, children put their feet much closer to each other, move more smoothly, which indicates an increase in their ability to balance the body.
Four-year-old children can change the rhythm of running, jumping. They can draw simple shapes and figures with a pencil, draw with paints, build structures from cubes. They can dress and undress independently, if the clothes are simple enough, serve themselves at the table. They learn to catch the ball, which indicates the development of their hand-eye coordination.
At this age, a new stage in the development of hand-eye coordination appears. At the age of 5, 30-50% of children already effectively use the mechanism of preliminary visual afferentation. The balance function at this age improves significantly, and children can walk on the balance beam, stand on one leg. Develops proper coordination of the movements of the arms and legs when walking.
At the age of 6-7 years, the maximum increase in running speed is observed, which is due not only to the improvement of movement control, but also to the growth of the lower extremities and increased flexibility of the joints. At the age of 6, a stable ability to make jumps is formed, pushing off with two legs. Fine motor skills also improve, so children can fasten and unfasten clothes. At the age of 6, motor skills in children are so developed that they begin to master professional activities - go in for sports, play musical instruments, dance, skate, etc.
The development of these skills requires training, and the main goal is to learn to do this without thinking, automatically.
The development of speech motor skills deserves special attention.
Speech is formed in a child gradually, along with his growth and development, and goes through a number of qualitatively different stages of development. The newborn may make involuntary sounds. They are innate, the same for children of all nations, despite the differences in languages and cultures. These sounds are the forerunners of speech. Speech sounds are special complex formations inherent only to humans. They are produced in a child within a few years after birth. This process includes complex brain systems and the periphery (speech apparatus), which are controlled by the central nervous system. Hazards that weaken development have a negative effect on the formation of pronunciation. The long way for a child to master the pronunciation system is due to the complexity of the material itself - the sounds of speech, which he must learn to perceive and reproduce. In the process of speech development, a child develops phonemic hearing, without which the appearance of speech is impossible. Phonemic hearing performs the operations of distinguishing and recognizing the phonemes that make up the sound shell of a word.
During the development of speech, systemically controlled auditory-motor formations are formed, which are real, material signs of the language. For their actualization, the existence of an articulatory base and the ability to form syllables are necessary. The articulatory base is the ability to bring the organs of articulation into positions necessary for the formation of the formation of sounds that are normative for a given language. In the process of mastering pronunciation skills and abilities, the child, under the control of his hearing and kinesthetic sensations, gradually finds and retains in memory those articulation modes that provide the necessary acoustic effect that corresponds to the norm. If necessary, these articulatory positions are reproduced and fixed. When finding the correct patterns, the child must learn to distinguish between articulation patterns that are similar in the pronunciation of sounds, and develop a set of speech movements necessary for the formation of sounds. As a rule, a child fully masters speech motor skills at the age of 4-5 years (by this age, sound pronunciation is fully formed), and mimic movements, which are lighter in their motor program, are assimilated in an earlier period of development.
Currently, the entire motor development of a child is considered according to the theory of dynamical systems: motor development involves many individual skills that are organized and, over time, reorganized to meet the requirements of certain tasks.
There are various definitions of dysarthria, however, the following definition of dysarthria has been highlighted in modern literature.
"Dysarthria - this is a violation of the pronunciation side of speech, due to insufficient innervation of the speech apparatus.
The main distinguishing feature of dysarthria from other pronunciation disorders is that in this case it is not the pronunciation of individual sounds that suffers, but the entire pronunciation side of speech.
The etiology of dysarthria as a symptom is not well understood. But as recent studies have shown, more than 80% of cases of this pathology are congenital disorders of the brain, that is, intrauterine disorders.
Specific causes leading to brain damage can operate in different periods: prenatal (basic), natal and postnatal.
But it is possible to single out some specific causes leading to brain damage and the occurrence of dysarthria in the prenatal (basic), natal and postnatal periods.
1) Prenatal period, that is, prenatal. The most common causes of intrauterine brain damage are: maternal diseases during pregnancy (viral, infectious); the mother has cardio-vascular and renal insufficiency; mental and physical trauma during pregnancy; increased dose of radioactivity during pregnancy; influence of nicotine, alcohol and drugs; mismatch between mother and fetus in terms of the Rh factor and group affiliation. The influence of these causes is especially dangerous in the first trimester of pregnancy.
2) Natal period (secondary aggravating factors): traumatic brain injury during childbirth; hemorrhage in the brain as a result of a sharp change in pressure (with rapid childbirth, with caesarean section); unsuccessful use of obstetrics (primary cause).
3) Postnatal period: diseases transferred by the child himself (meningitis, meningo-encephalitis and others); traumatic brain injury.
It is important to note that prenatal distress often entails distress in the natal and postnatal periods.
The most common classification of dysarthria in Russian speech therapy was created taking into account the neurological approach based on the level of localization of the lesion of the motor apparatus of speech.(O.V. Pravdina and others). There are the following forms of dysarthria: bulbar, pseudobulbar, extrapyramidal (or subcortical), cerebellar, cortical.
The main symptoms of dysarthria are defects in sound pronunciation and voice, combined with speech disorders, especially articulatory motility and speech breathing.
In addition to this, in symptoms of dysarthriaidentify verbal and non-verbal symptoms. TOnon-speech include: massive violations of the motor apparatus or motor sphere; violation of the emotional-volitional sphere; violation of cognitive activity; peculiar formation of personality; violation of articulation, breathing, muscle tone.
Motor disorders usually appear at later stages of the formation of motor functions, especially such as the development of the ability to sit down independently, crawl with alternate simultaneous extension of the arm and the opposite leg and with a slight turn of the head and eyes towards the extended arm, walk, grab objects with the fingertips and manipulate them.
Emotional-volitional disorders are manifested in the form of increased emotional excitability and exhaustion of the nervous system. In the first year of life, such children are restless, cry a lot, require constant attention. They have sleep disturbances, appetite, predisposition to regurgitation and vomiting, diathesis, gastrointestinal disorders. Such children, as a rule, are weather dependent.
At preschool and school age, they are motorally restless, prone to irritability, mood swings, fussiness, often show rudeness, disobedience. Motor restlessness increases with fatigue, some children are prone to reactions of the hysteroid type.
Despite the fact that children do not have pronounced paralysis and paresis, their motor skills are characterized by general awkwardness, lack of coordination, they are awkward in self-service skills, they lag behind their peers in dexterity and accuracy of movements, they have a delay in developing hand readiness for writing, therefore, for a long time there is no interest in drawing and other types of manual activities, poor handwriting is noted at school age. Disorders of intellectual activity are expressed in the form of low mental performance, memory and attention disorders.
Many children are characterized by a slow formation of spatio-temporal representations, optical-spatial gnosis, phonemic analysis, and constructive praxis.
TO speech symptomsinclude: violation of sound pronunciation; violation of the prosodic side of speech; violation of phonemic functions. Fuzzy, slurred speech does not allow the formation of a clear auditory image of the word, which in turn further exacerbates sound pronunciation defects; violation of the lexical and grammatical structure of speech; reading and writing impairment.
Thus, dysarthria are the most common speech disorders in children. Clinical features and severity of disorders depends primarily on the location and severity of brain damage.
It should be emphasized that the diagnosis is made jointly by a doctor and a speech therapist. Unfortunately, practicing neurologists do not pay attention to determining the form of dysarthria when making a diagnosis, limiting themselves to the wording “dysarthria” or “erased form of dysarthria” (“dysarthria component”).
Thus, the lack of formation of the psychophysiological prerequisites for the development of the phonetic side of speech at the sensorimotor level, the interdependence of speech and non-speech processes, the features of the structure and mechanisms of phonetic disorders determine the main directions of corrective action: the development of speech-auditory perception and phonemic functions, fine and articulatory motor skills; correction of sound pronunciation disorders.
Children with speech disorders are children who have deviations in the development of speech with normal hearing and intact intelligence. Speech disorders are diverse, they can manifest themselves in violation of pronunciation, grammatical structure of speech, poverty of vocabulary, as well as in violation of the pace and fluency of speech.
Dysarthria (from the Greek dys - a prefix meaning a disorder, arthroo - articulately pronounce) - a violation of pronunciation due to insufficient innervation of the speech apparatus in cases of lesions of the posterior frontal and subcortical regions of the brain.
The founders of the doctrine of dysarthria, defining the ways of clinical and pedagogical rehabilitation, recommended an integrated approach to corrective measures.
This comprehensive approach to the elimination of dysarthria includes three blocks.
The first block is medicaldetermined by a neurologist. In addition to medications, exercise therapy, massage, reflexology, physiotherapy, etc. are prescribed.
The second block is psychological and pedagogical. The main direction of this impact will be the development of sensory functions.
The third block - speech therapy workwhich is carried out mainly on an individual basis.
The implementation of an integrated approach to the correction of motor disorders in children with dysarthria will be effective if the following conditions are met:
The speech therapist is working purposefully on the development of general, speech and fine motor skills of the fingers;
The entire teaching staff of the preschool educational institution and the parents of the pupils take part in the correction process.
Directions of corrective work on the development of motor functions in older preschoolers
Blocks | |
Medical (on the basis of a medical institution - a children's clinic) | Pedagogical (based on DOW) |
Directions | |
drug treatment | Correction of speech motor skills |
physiotherapy | General motor correction |
massage (general) | Correction of fine motor skills of fingers |
exercise therapy |
The implementation of a set of measures within the framework of pedagogical influence provides for the close interaction of all participants in the correctional and developmental process: a speech therapist, educators, a child, parents, and the entire teaching staff of the preschool educational institution.
It is necessary to regularly carry out articulation gymnast complexes, which are widely known to S.E. Bolshakova, V.A. Kiseleva, A.R. Luria, T.V. Volosovets. Articulation gymnastics should be carried out both by the speech therapist himself and by the group educators, parents with children as part of homework.
In the classroom, a speech therapist and educators should offer children various static and dynamic exercises for the development of finger motor skills. In many cases, they can be supported by the poetic text of V.B. Galkina, V.P. Dudiev, M.M. Koltsova, I.S. Lopukhina, E.V. Novikov.
Also used are various didactic games(lacing, laying out letters from sticks, puzzles, hatching, etc. A.E. Belaya, A.R. Luria, which were accompanied by speech games.
Classes in logopedic rhythm G.A. Volkova, N.V. Nishcheva, O.V. Pravdina is also necessary for this contingent of children. These classes are held jointly by the music director and speech therapist (once a week a physical education instructor is included in the process).
Physical minutes in the classroom serve both for the physical and psychological unloading of children, and for the development of their motor skills, mental processes.Usually a physical minute is an exercise for the hands, less often - tilts or squats. The work usesquestion-answer games with the ball, the execution of commands according to instructions, etc.
In the classes, a speech therapist and educators use a neuropsychological technique developed by V.A. Kiseleva together with A.V. Semenovich, aimed at correcting the motor sphere of preschoolers - dysarthria. The methodology involves work within the following sections: developmentspeech motor skills, development gross motor skills and fine motor skills of the fingers.
Musical classes, as well as physical education, contribute to the development of the motor sphere.
Of great benefit are classes that are in the competence of educators - modeling, designing, drawing.
The speech therapist also conducts remedial classes in the form of recommendations to parents.
Blocks | Techniques | Saturation |
motor sphere | 1. Development of tactile sensations of a motor act. 2. Development of the kinesthetic component of the motor act. 3. Dynamic coordination of movements. | Development of fine motor skills - Hand movements Finger movements - Exercises performed with both hands together. Movements are performed with one hand, the other, then both hands at the same time |
"Fingers say hello." "Who will win." "Sun". "Swamp". |
||
Articulation gymnastics | For mimic muscles For lips For language Move your tongue from side to side, then put it back in your mouth |
|
Mimic and articulation exercises | Mimic exercises Removal of spasticity and reduction of salivation Articulation gymnastics 1. Exercises for the lower jaw 2. Lip exercises 3. Language exercises |
|
Development of spatial representations | Synthesis of finger gymnastics with articulation exercises (according to V.A. Yastrebova and O.I. Lazareva) | lower jaw training Lip muscle training Tongue muscle training |
Fizminutka |
Children with dysarthria do have problems in the motor sphere, therefore, a system of exercises is needed to overcome these disorders and the implementation of an integrated approach in the correctional and educational process. One of the important conditions for effective work is the participation in the process of correction of the entire teaching staff of the preschool educational institution and the parents of pupils.
BIBLIOGRAPHY
- Anokhin PK Essays on the physiology of functional systems. - M.: Medicine., 1975. - 477 p.
- Arkhipova, E.F. Clinical and pedagogical characteristics of children with an erased form of dysarthria [Text]: Study method. allowance / E.F. Arkhipova. – M.: AST: Astrel, 2008. – 254 p.
- Belaya, A.E. Finger games for the development of speech of preschoolers [Text] / A.E. White. – M.: Vlados, 1999. – 48 p.
- Bolshakova, S.E. Speech disorders and their overcoming. Collection of exercises [Text] / S.E. Bolshakov. - M.: TC Sphere, 2005. - 128 p.
- Bernstein N.A. Essays on the physiology of movements and the physiology of activity. – M.: Medgiz, 1966. – 234 p.
- Vinarskaya, E.N. Dysarthria [Text] / E.N. Vinarskaya. - M.: Astrel, 2005. - 141 p.
- Vinarskaya, E.N., Bogomazov G.M. Age phonetics [Text] / E.N. Vinarskaya, G.M. Bogomazov. - M.: Astrel, 2005. - 144 p.
- Vlasova, T.A., Pevzner, M.S. About children with developmental disabilities [Text] / T.A. Vlasov. M.S. Pevzner. - M.: Enlightenment, 1973. - 173 p.
- Volkova, G.A. Logopedic rhythm[Text] / G.A. Vlasov. - M.: Vlados, 2003. - 272 p.
- Volkova, G.A. Methods of psychological and logopedic examination of children with speech disorders. Issues of differential diagnosis [Text]: Textbook-method. allowance / G.A. Vlasov. - St. Petersburg. Detstvo-Press: 2004.- 144 p.
- Vygotsky L.S. Thinking and speech: Psychological research. -M.: Labyrinth, 1966. - 416 p.
- Gavrina, S.E. We train the hand: workbook [Text] / S.E. Gavrina. – M.: Rosmen-Press, 2001. – 20 p.
- Galkina, V.B. The use of physical exercises for the development of fine motor skills of the fingers in the correction of speech disorders in primary school students [Text] / V.B. Galkin. // Defectology. - 1999. - No. 3. p.37
- Golubeva, G.G. Correction of violations of the phonetic side of speech in preschoolers [Text] / G.G. Golubev. - St. Petersburg: RGPU im. Herzen, 2000. - 62 p.
- Zhinkin, N.I. Mechanisms of speech [Text] / N.I. Zhinkin. - M .: Education, 1990. - 370 p.
- Zaitseva, L.A., Zaitsev, I.S., Levyash, S.F., Yasova, I.N. Disorders of the pronunciation side of speech and their correction [Text]: Study method. Allowance / L.A. Zaitseva, I.S. Zaitsev, S.F. Levyash, I.N. I am an owl. - Minsk: BSPU im. M. Tanka, 2001. - 74 p.
- Zeeman, M. Speech disorder in childhood [Text] / Per. from Czech. E.O. Sokolova. // Ed. VC. Trutkeva, S.S. Lyapidovsky. – M.: Medgiz, 1962 – 299 p. Lalaeva, R.I. Formation of vocabulary and grammatical structure in preschool children with general underdevelopment of speech [Text] / R.I. Lalaeva, N.V. Serebryakova - St. Petersburg. : Soyuz, 2001. - 224 p.
- Lalaeva, R.I. Formation of vocabulary and grammatical structure in preschool children with general underdevelopment of speech [Text] / R.I. Lalaeva, N.V. Serebryakova - St. Petersburg. : Soyuz, 2001. - 224 p.
- Kiseleva, V.A. Diagnosis and correction of the erased form of dysarthria. [Text] / V.A. Kiseleva. - M .: School press, 2007 - 48 p.
- Koltsova, M.M., Ruzina, M.S. The child learns to speak [Text] Finger game training / M.M. Koltsova, M.S. Ruzina. - St. Petersburg: MiM, 1998. - 190p.
- Kornev, A.N. Fundamentals of childhood speech pathology [Text]: clinical and psychological aspects / A.N. Kornev. - St. Petersburg: Speech, 2006 378. p.
- Leontiev, A.A. Fundamentals of psycholinguistics. [Text] / A.A. Leontiev. – M.: Meaning, 1999.- 287 p.
- Speech therapy service: problems, search [Text] - Murmansk, 2000.
- Speech therapy [Text]. methodological legacy. In 5 books. Book. I: Violations of the voice and the sound-producing side of speech: At 2 pm Part 2 .: Rhinolalia. Dysarthria / Ed. L.S. Volkova. - M., 2006. - 303 p.
- Lopatina, L.V. The study and correction of psychomotor disorders in children with minimal dysarthric disorders [Text] / L.V. Lopatin. // Defectology. - 2003. - No. 5. - c. 45-51.
- Lopatina, L.V., Serebryakova, N.V. Overcoming speech disorders in preschoolers (Correction of erased dysarthria). [Text] / L.V. Lopatina, N.V. Serebryakova. - St. Petersburg: Peter, 2001. 190 p.
- Lopatina, L.V. Speech therapy work with preschool children with minimal dysarthria disorders: Proc. allowance [Text] / L.V. Lopatin. - St. Petersburg: Soyuz, 2004. - 191 p.
- Lopukhin, I.S. speech therapy. Speech, rhythm, movement. [Text] / I.S. Lopukhin - 2nd ed. - St. Petersburg: Korona print, 2004. - 128s.
- Luria, A.R. Fundamentals of neuropsychology. [Text] / Proc. allowance for students. higher textbook establishments. / A.R. Luria - M .: Publishing Center "Academy", 2003. - 384 p.
- Mastyukova, E.M. Curative pedagogy (early and preschool age): Tips for teachers and parents on how to prepare children with special developmental problems for teaching. [Text] / E.M. Mastyukov. - M.: Vlados, 1997.– 304 p.
- Methods for examining the speech of children. Manual for the diagnosis of speech disorders [Text] / Ed. G.V. Chirkina. - M., 2005. - 240 p.
- Nishcheva, N.V. The system of correctional work in a speech therapy group for children with general underdevelopment of speech. [Text] / N.V. Nishchev. - St. Petersburg: Detstvo-Press, 2000. - 112 p.
- Novikova, E.V. Probe massage: correction of fine motor skills of the hand: A visual and practical guide [Text] / E.V. Novikov. - M.: "Izd. Gnome and D", 2004. - 80 p.
- Novikovskaya, O.A. The development of sound culture of speech in preschoolers [Text] / OA Novikovskaya. - M .: Childhood-Press, 2002. - 48 p.
- Fundamentals of speech therapy with a workshop on sound pronunciation [Text]: Proc. allowance for students. avg. ped. studies, institutions / M.F. Fomicheva, T.V. Volosovets, E.N. Kutepova. / Ed. T.V. Volosovets. - M.: M.: Publishing Center "Academy", 2002. - 200 s.
- Fundamentals of speech therapy work with children [Text] / Ed. G.V. Chirkina. - M .: Pedagogy, 2002. - 240 p.
- Pravdina, O.V. Speech therapy [Text] Textbook. manual for students defectologist. facts ped. in-comrade. Ed. 2nd, add. and reworked. / O.V. Pravdin. - M.: Enlightenment, 1973. - 272 p. C84
- Pravdina - Vinarskaya, E.N. The current state of the problem of dysarthria [Text] / E.N. Pravdina - Vinarskaya. - M.: Enlightenment, 1973. - 283p.
- Prikhodko, O.G. Speech therapy massage in the correction of dysarthria disorders in children of early and preschool age [Text] / O.G. Prikhodko. - St. Petersburg: KARO, 2008. - 157 p.
- Reader on speech therapy [Text] / Ed. Volkovoy L.S., Seliverstova V.I. - M.: Vlados, 1997. - S.227-228, 238-243.
- Rozhkova, L.A., Peresleni, L.I. Neurophysiological criteria for assessing the level of development of mechanisms of cognitive activity in children in the aspect of problems of differential diagnosis [Text] / L.A. Rozhkova, L.I. Move over. // Defectology. - 2001. - No. 4. - C.4.
- DEVELOPMENT OF TACTILE SENSATIONS AND KINESTHETIC COMPONENT.
MOTOR ACT
We start by teaching the child the techniques of self-massage of hands. Self-massage is one of the types of passive gymnastics, it must be carried out daily, preferably 2-3 times a day. It has a tonic effect on the central nervous system, improves the function of receptors, pathways. Self-massage begins with light rubbing of the fingertips in the direction from the tips to the palm of one hand, then the other. Next, the palm of one hand is rubbed from the middle to the edges with the thumb of the other hand. After that, a set of exercises is carried out.
"Dotted lines". The pads of the four fingers of the right hand are located at the bases of the fingers of the left hand on the back of the palms. With back and forth movements (“dotted lines”) we shift the skin, gradually moving towards the wrist joint. The same on the other hand.
"Saw". The left hand (hand and forearm) lies on the table with the palm up. With the edge of the right palm, we imitate the movement of the saw along the entire surface of the left palm in the up and down direction. The same for the other hand.
"Iron". The starting position (I.p.) is the same. Stroking with the right hand, rubbing, kneading the left. The same for the other hand.
"Ice rink". I. p. the same. With the knuckles of the fingers of the right hand clenched into a fist, we move up and down the left palm, kneading it. The same for the other hand.
* Exercises marked with this icon are performed in combination.
"Gimlet". I.p. also. With the phalanxes of the fingers of the right hand clenched into a fist, we make movements like a “gimlet” on the left palm. The same for the other hand.
"Crab". I.p. the same, fingers apart. We bend the index and middle fingers of the right hand and pinch the fingers of the left with the phalanges. The same for the other hand.
"Warm your hands." We rub our hands vigorously.
"Spirals". Each finger of the left hand alternately, starting with the little finger, is placed on the four fingers of the right hand. With the thumb of the right hand, we make spiral movements along the finger of the left from the bottom up from the base to the pad. The same for the other hand.
After performing self-massage, you can proceed to the following exercises.
1. "Hot - warm - cold." The child should by touch compare and determine the degree of heating of objects (heater - ice - soft toy- a metal spoon ...).
2. "Find what it's made of." The child first feels 3-5 toys with different surface textures, then pieces of the materials from which the toys are made. It is necessary to relate to the touch the toy and the material from which it is made.
3. "Pool for fingers." Pour peas (beans, buckwheat, rice) into a large box with sides 7-8 cm high and place several objects, different in shape and size, familiar to the child. He must lower his hands into the "pool", find objects, feel them and name them.
4. "Magic bag". 1st option. The child must guess by touch what is in the bag:
a) household items (pencil, coin, ring...);
b) small toys; v) geometric figures various sizes and textures (sandpaper, velvet paper, thick foil); d) letters and numbers, different in size and texture (for children familiar with them). 2nd option. The child is invited to feel the object with one hand, then: a) examine the drawings of objects and choose the same one from them; b) draw the same object; c) choose among others the same object with one, then with the other hand.
2. DEVELOPMENT OF THE KINETIC COMPONENT
MOTOR ACT
Hand movements
Movements are performed according to the pattern, first with one hand, then with the other hand, and finally with both hands at the same time.
1. Rolling the ball (tennis ball) on an inclined plane with the palm of your hand.
2. Squeezing rubber toys, syringes filled with water (with a given direction of air or water jet).
3. Hit the balloon suspended from the ceiling (fist, palm, index finger).
4. "Funny painters." The elbows rest on the table, the fingers are extended and tightly pressed to each other, the brushes move up and down.
5. "Cowardly bunny." The elbows rest on the table, the index and middle fingers are extended and spread apart, the rest are tightly pressed to the palm, movements are made with the brushes in the up and down direction.
6. "The hen drinks water." The elbows rest on the table, all the fingers are extended and gathered into a “beak”, movements are made with the brushes in the up and down direction.
7. "Goose". The elbows rest on the table, the thumb and forefinger are extended and tightly pressed to each other, the rest are pressed to the palm, movements are made with the brushes in the up and down direction.
8. "Cockerel". The elbows rest on the table, the thumb and forefinger form a “beak”, the rest are laid on the index finger, movements are made with the brushes in the up and down direction.
9. "Let's pet a kitten." The elbows rest on the table, the fingers are extended and tightly pressed to each other, the brushes are moved in the direction left and right.
10. "Goat butted." The elbows rest on the table, the index finger and little finger are extended and spread apart, the rest are tightly pressed to the palm, movements are made with the brushes in the left-right direction.
11. "Checkbox". The elbows rest on the table, the fingers are tightly pressed to the palm, except for the thumb, which is protruded and directed upwards, movements are made with the brushes in the left-right direction.
12. "Good-bad." The elbows rest on the table, the fingers are tightly pressed to the palm, except for the thumb, which is protruding and points up - “good”, then down - “bad”.
13. Wasps. The elbows rest on the table, the index finger is extended, the rest are tightly pressed to the palm, movements are made with the brushes in a circle.
Finger movements
Movements are performed according to the pattern, performed with one hand, the other hand, then with both hands at the same time.
1. "Beetle". The elbows rest on the table, the index finger is extended, the remaining fingers are tightly pressed to the palm, the movements are made with the index finger in a circle - the beetle flies. Similarly, the exercise is carried out with other fingers.
2. "Snake". The elbows rest on the table, the index finger is extended, the remaining fingers are tightly pressed to the palm, the movements are made with the index finger, imitating the movements of the snake. Similarly, the exercise is carried out with other fingers.
3. "Bunny". The elbows rest on the table, the index and middle fingers are extended and directed upwards, the remaining fingers are tightly pressed to the palm, the movements are made with outstretched fingers - the bunny moves its ears.
4. "Goat". The elbows rest on the table, the index finger and little finger are extended and directed forward away from you, the remaining fingers are tightly pressed to the palm,
movements are made with outstretched fingers - the goat butts.
5. "Goat". The elbows rest on the table, the thumb and little finger are extended and directed forward from themselves, the remaining fingers are tightly pressed to the palm, movements are made with outstretched fingers - the goat is butting.
6. "Cat". The elbows rest on the table, the index finger and little finger are extended and slightly bent, the middle and ring fingers are tightly pressed with the thumb to the palm, the movements are made with outstretched fingers - the ears move.
7. "Keg". Elbows rest on the table, fingers, except for the thumb, are tightly pressed against each other and close with the palm, movements are made with the thumb - the barrel opens - closes.
8. "Flower". The elbows rest on the table, the fingers are tightly pressed to each other, the palm is pointing up, the fingers slowly open.
9. "Frog". The elbows rest on the table, the index finger and little finger are bent and pulled back, the middle and ring fingers are firmly pressed to the palm, the thumb is attached to them horizontally. Movements are made with the index finger and little finger - the frog is sleeping - woke up.
10. "Crocodile". The elbows rest on the table, the index finger and little finger are bent and pulled back, the middle and ring fingers are stretched forward, the thumb is pressed against them from below - the mouth. Movements are made with outstretched fingers - the crocodile "eats".
11. "Snail". Put your hands on the table, raise your index and middle fingers, the rest are firmly pressed to the table. Raised fingers move - the snail moves its horns.
12. "Owl". The elbows rest on the table, the index, middle and ring fingers are bent so that the pads are pressed to the base of the fingers, the thumb and little finger stick out to the sides. They make movements - the owl flies.
Additionally, you can use the sorting of cereals, buttons, beads, etc.; lacing; work with plasticine, clay, scissors; origami.
Exercises performed with two hands together
1. "Ladle". Both palms are connected by ribs on the table, the fingertips of the left and right hands touch, the thumbs are pressed to the index fingers.
2. "Steamboat". Both palms are connected by ribs on the table, the fingertips of the left and right hands are touching, the thumbs are protruding upwards - the pipe of the steamer.
3. "Nest with eggs." Both hands are connected in the same position as in the previous exercise, but the thumbs are lowered inward.
4. "The roof of the house." The elbows rest on the table, the palms are directed upwards, the fingers of both hands are tightly pressed and touch with pads, the brushes are maximally apart.
5. Birdhouse. The elbows rest on the table, the palms are directed upwards, the fingers of both hands are slightly bent and touch the pads, the thumbs are bent inside the palms.
6. "Points". The elbows rest on the table, the fingers of both hands are gathered into a ring and connected.
7. "Gate". The elbows rest on the table, the palms are directed upwards, the pads of the middle and ring fingers of both hands are connected, the index fingers and little finger are straightened, the thumbs are tightly pressed to the index fingers.
8. "Bridge". The elbows rest on the table, the middle, ring and little fingers of both hands are tightly pressed and connected horizontally with pads, the index fingers are extended upwards, the thumbs are pressed to them.
9. Roots. The elbows rest on the table, the palms are pressed with the back side, the fingers are lowered down.
10. "Mill". The elbows rest on the table, the palms are directed upwards, the fingers of both hands are extended and intertwined. Movements are made with outstretched fingers, without disengaging them - the mill works.
11. "Basket". The palms are directed towards themselves, the fingers of both hands are intertwined inside the palms, the thumbs are closed in a ring.
12. "Bell". The elbows rest on the table, the palms are directed upwards, the fingers of both hands are intertwined, the middle finger of the right hand is lowered down - the tongue of the bell.
3. DYNAMIC COORDINATION OF MOVEMENTS
Movements are performed with one hand, the other hand, then both hands at the same time.
1. "Cam". The hand lies on the table with the back side. We alternately squeeze our fingers into a cam, starting with the thumb, and unclench, starting with the little finger.
2. "Hello, finger." Elbows rest on the table, all fingers alternately touch the big pads - they say hello.
3. "The man is running." The index and middle fingers are straightened, the rest are pressed to the palm with the thumb. Straightened fingers move on the table.
4. "Binoculars". The elbows rest on the table, the palms are raised up, the thumbs are connected horizontally. The remaining fingers, starting with the index finger, are alternately attached to the thumbs (hand movements can be either simultaneous or sequential) until the formation of "binoculars".
5. "Bear clubfoot." All fingers, except the middle one, are on the table, the middle one is bent and raised up - the bear's head. They perform movements alternately with the thumb and forefinger - the ring and little fingers, as if imitating the gait of a bear.
6. "Playing the piano." The palms rest on the table in the pianist's position (fingers slightly bent). Alternately tapping with the first - second, first - fifth fingers.
7. "Crab". The palms are pointing down, the fingers are interlaced inward, the thumbs are directed towards themselves.
"Crab" moves on the table left and right by alternately rearranging the thumb of the right hand - the remaining fingers of the right hand - the thumb of the left hand - the remaining fingers of the left hand.
4. DEVELOPMENT OF RECIPROCAL COORDINATION OF HAND MOVEMENTS
1. "Chair". Elbows rest on the table. The left palm is raised vertically upwards, the fingers are tightly clenched. The right hand is bent into a fist and placed on the lower part of the palm of the left hand, then the position of the hands changes.
2. "Table". The left hand, bent into a fist, stands on the edge of the table. The right hand is straightened, covering the top of the left. Then the position of the hands changes.
3. "Pointer". The elbow of the left hand rests on the table, the palm is turned towards itself, the fingers are folded into a fist, the thumb is set aside. The right hand is straightened, palm down, fingers tightly pressed. The fingers of the right hand touch in a horizontal position to the base of the little finger of the left hand. Then the position of the hands changes.
4. "Chicks". The left hand lies on the table, palm up, fingers pressed and straightened up. Grasp the fingers of the left hand with the right hand. Then the position of the hands changes.
5. "Hide and Seek". The elbows rest on the table, the palms are pressed with the back. The left hand is bent into a fist and is behind the right (hiding), the palm of the right hand is straightened. Then the position of the hands changes.
6. Drawing. At the same time, twists are drawn with one hand, and squares with the other.
7. Imitation of playing the piano, guitar, balalaika, violin, etc.
For children of the second and third groups (with an average and severe severity of violations), we recommend adding "Colorful clothespins" at the 2nd and 3rd stages. Plastic clothespins are fixed during the exercises on the fingers lasting from 3 to 10 minutes according to the scheme:
1-3rd day - thumb;
4-6th day - thumb and forefinger;
7th day - thumb, index and middle fingers;
10-12th day - thumb, index fingers;
13-15th day - thumb.
On days not indicated in the scheme, clothespins do not need to be attached.
FINGER GAMES
- Alternately touch the thumb of the right hand to the second, third, fourth and fifth fingers at the usual and maximum pace. (Then with the right hand; with both hands.)
- With the fingers of the right (left) hand, “say hello” in turn with the fingers of the left (right) hand (patting the fingertips, starting with the thumb).
- "Fingers say hello."
Connect fingers. To carry out alternately, starting with the thumb, touching movements of all fingers.
- "Who will win."
Connect the hands in front of you. Alternately make hand presses to the right, to the left. Spread the fingers of the right (left) hand wide, bring them together, spread them again, hold for 2-3 seconds.
- "Sun".
Put the palm of the right (left) hand with spread fingers-rays on the table. Make alternate tapping with your fingers on the table.
- "Swamp".
The thumb of the right (left) hand is set on the "bump". The remaining fingers alternately "jump from bump to bump." (Similar movements are carried out starting with the little finger.)
Section 2. Mimic and articulation exercises.
ARTICULATION GYMNASTICS
For mimic muscles
- “Angry” - frown.
- “Surprised” - raise your eyebrows up.
- “Day” - “Night” - calmly open and close your eyes.
- “Fatties” - puff out your cheeks.
- "Thin" - draw in the cheeks.
- “Fatties” - “Thin” - first inflate, then draw in your cheeks.
For lips
- “Chick”, “Window” - the mouth is wide open, the tongue lies quietly in the oral cavity.
- “Smile” - lips are kept in a smile. Teeth are not visible.
- “Fence” - lips are pushed forward with a long tube.
- “Proboscis” - pull closed lips forward.
- “Doughnut”, “Speaker” - teeth are closed. Round the lips and slightly stretch forward so that the upper and lower incisors are visible.
- “Fence”, “Donut”, “Smile”, “Proboscis” - alternate the position of the lips.
- "Rabbit" - teeth are closed. Raise the upper lip and expose the upper incisors.
- “Comb” - “comb” the lower lip with the upper teeth, like a comb, and vice versa, “comb” the upper lip with the lower teeth.
For language
- “Automatic”, “Machine gun” - close your mouth. With a tense tip of the tongue, knock on the teeth, repeatedly and distinctly pronouncing: “t - t - t”. Accelerate the pace gradually.
- “Drummer”, “Woodpecker” - smile, open your mouth and tap your upper incisors with the tip of your tongue, repeatedly and distinctly pronouncing: “d - d - d”.
- “Delicious jam” - open your mouth. Lick the upper lip with a wide tongue and remove the tongue deep into the mouth.
- “Funny snake” - stick out the tongue from the mouth, then put it back into the mouth.
Move your tongue from side to side, then put it back in your mouth
- "Accordion" - close your mouth. Rest the tip of the tongue against the lower incisors, lift the back of the tongue up.
- "Fungus" - open your mouth. Stick your tongue to the sky.
- “Turkey” - open your mouth, move the wide front edge of the tongue along the upper lip back and forth, trying not to tear the tongue from the lip, add a voice until you hear: “bl - bl ...” (like a turkey chattering).
- “Needle”, “Arrow”, “Sting” - open your mouth. Push a narrow tense tongue forward.
- “Swing” - open your mouth. With a tense tongue, reach for the nose and chin, or for the upper and lower incisors.
- “Coil” - open your mouth. Rest the tip of the tongue against the lower incisors, press the lateral edges against the upper molars. Wide tongue “roll out” forward and remove deep into the mouth.
- “Ladle” - open your mouth wide. Put a wide tongue on the lower lip. Bend the tip and sides so that you get a deepening of the back of the tongue. Bring the “dipper” into your mouth, lifting the tip of your tongue to the tubercles.
- “Scapula” - open your mouth, put a wide, relaxed tongue on your lower lip.
- “Horse” - smile and open your mouth. Click slowly with the tip of the tongue. Make sure that the lower jaw and lips do not move, but only the tongue works.
- "Malyar" - open your mouth. With a wide tip of the tongue, like a brush, lead from the upper incisors to the soft palate.
- “Naughty tongue” - open your mouth, put your tongue on your lower lip and, slapping it with your lips, say: “five-five-five…”
- “Let's lick lips”, “Pussy licks” - open your mouth slightly. Lick first the upper, then the lower lip in a circle.
- “Brush your teeth” - close your mouth. In a circular motion of the tongue, draw between the lips and teeth.
- “Let's count the lower teeth” - smile, open your mouth. With the tip of the tongue, rest in turn on each lower tooth. The jaw does not move.
- “Let's brush the lower teeth” - smile, show your teeth, open your mouth and “clean” the lower incisors with the tip of your tongue, first moving your tongue from side to side, then from bottom to top.
- “Glue the candy” - put a wide tongue on the lower lip. Put a thin piece of toffee on the tip of the tongue, glue the candy to the sky behind the upper incisors.
- “Steps” - open your mouth slightly, “hug” your upper lip with the wide end of your tongue - this is the first step; hug the upper teeth with a wide tip of the tongue - this is the second; press the wide tip of the tongue to the upper tubercles - the third.
- “Tube”, “Groove” - open your mouth. Bend the sides of the tongue up.
- “Football”, “Hide the candy” - close your lips. With a tense tongue, rest against one or the other cheek.
- “Watch”, “Pendulum” - open your mouth. Stretch your lips into a smile. With the tip of a narrow tongue, alternately stretch under the teacher's account to the corners of the mouth.
- "Bumblebee" - open your mouth. Raise the tongue in the form of a cup, press the lateral edges to the molars. The leading edge must be free. In the middle of the tongue, start an air stream, connect your voice, pronouncing with force: “zzzz”, “jzhzh”.
- “Tongue is a strongman” - smile slightly, open your mouth, lower the tip of your tongue to the lower front teeth and rest your tongue against your teeth.
- “Tongue on the balcony” - open your mouth slightly, “hug” the upper lip with the wide end of the tongue.
- “The tongue dries the tail” - relax the tongue, hang it on the edge of a clean spoon and blow on its tip with force.
MIMIC AND ARTICULATION EXERCISES
Mimic exercises
Before performing the exercises, a massage (self-massage) of the face is performed. With warm 2, 3, 4 fingers, folded together, stroke the face in the directions: from the base of the neck to the chin, starting from the middle part of the neck, from the middle of the chin to the earlobes, from the corners of the lips to the tragus of the ears, from the nose to the temples, from the middle of the forehead to the temples. Then kneading, pinching, patting is carried out in the same directions. The massage ends with light patting of the face with the pads of four fingers.
Then facial exercises are performed, such as: frown the forehead, eyebrows, close both eyes, one eye, wink, puff out the cheeks, move air from one cheek to another, etc.
Removal of spasticity and reduction of salivation
The work of a speech therapist is greatly complicated by increased salivation in a child with an erased form of dysarthria. It is desirable to include a set of exercises to relieve spasticity and reduce salivation in the work, anticipating articulation exercises, so that by the time the articulation gymnastics begins, there are no additional difficulties.
Soft palate massage - stroking and kneading finger movements along the midline of the hard and soft palate from the upper incisors to the Uvula to obtain a pronounced pharyngeal reflex.
Applying a piece of ice along the contour of the lips (6 points) (Fig.). The duration of ice retention at each point is from 5 seconds to 1 minute.
Rinsing the mouth with the use of medicinal herbs: infusion of wild rose, oak bark, yarrow (you must first make sure that the child does not have allergies).
Gargling in stages: mineral water, liquid jelly, kefir, thick jelly.
Rice. Points on the upper and lower lip for applying ice
Throwing your head back, imitate rinsing movements.
Throwing your head back, imitate chewing movements.
Throw back your head, yawn.
Put a bread ball on the tip of the tongue (crushed vitamins, drip 1-2 drops of syrup from the pipette), with an effort to make a swallowing movement.
Pronunciation of vowels a, e, and on a hard attack: a a a; uh uh; and and and;
ae ae ae; ea ea ea; ai ai ai; Hey Hey hey; aei aei aei.
Point massage. Find parallel points under the tragus of the ears, where the jaw bones meet (correctly found points are painful). With index fingers do circular motions points for 5 minutes clockwise (2.5 minutes - with an open mouth, 2.5 minutes - with a closed one) and 5 minutes counterclockwise (similarly).
Articulation gymnastics
Each speech therapist in the arsenal has a large supply of various articulation exercises. You can supplement them with exercises borrowed from acting practice.
1. Exercises for the lower jaw
The chin is in the usual comfortable position, the lips are closed. At the count of “one”, the jaw drops to a distance of the width of two fingers, the tongue lies freely, the tip of the tongue is at the lower incisors, the lips retain a rounded shape, the teeth are not exposed. At the expense of "two", the open position of the mouth is fixed. On the count of three, the mouth is closed. The exercise is repeated six times in a row. Care must be taken not to tilt the head.
I.p. also. At the expense of "one" the jaw moves forward; at the expense of "two" the jaw takes its original position; on the count of "three" the jaw drops; on the count of "four" the jaw moves forward; at the expense of "five" the jaw takes its original position. Movements are repeated 4-5 times at a slow pace.
I.p. also. At the count of "one" the jaw drops; at the expense of "two" the jaw moves to the right (the mouth is open); on the count of three, the jaw drops again; on the count of "four" the jaw moves to the left; on the count of "five" the jaw drops, on the count of "six" the jaw moves forward; at the expense of "seven" the jaw returns to its original position. Movements are repeated 2-3 times at a slow pace.
2. Lip exercises
Before doing exercises, you need to massage your lips.
Place both index fingers on the upper lip (points located on both sides between the corner of the mouth and the middle of the lip). We perform stroking
movements with two fingers simultaneously towards the middle of the lip (4-5 times). The same on the lower lip.
I.p. too. We perform stroking movements in the upward direction, exposing the gums (4-5 times). The same on the lower lip (downward direction).
Put your index fingers on the corners of your mouth. We stretch the lips to the sides (“smile”), we collect the lips together (“proboscis”).
The lips are in the usual relaxed position. We perform light pinching first of the upper, then of the lower lip with the index and middle fingers of both hands in the direction from the middle of the lips to the corners of the mouth.
I.p. also. We perform light tapping of both lips with the index and middle fingers of both hands in the direction from the middle of the lips to the corners of the mouth.
I.p. also. We make light stroking movements of both lips with the index and middle fingers of both hands in the direction from the middle of the lips to the corners of the mouth.
After the massage, you can proceed to the exercises (movements are repeated 4-5 times), starting with holding the static posture "smile", "tube", "proboscis" for 3-10 seconds.
Grab a napkin with your lips, try to prevent it from being removed from your mouth.
I.p. - the mouth is closed, the teeth are closed, the lips are in the usual position. Raise and lower the upper lip to the count of "one, two." The same with the lower lip.
I.p. also. At the same time, at the expense of “times”, raise the upper lip, lower the lower; on the count of "two" lower the upper lip, cover it with the lower one.
I.p. also. On the count of "one" the lower lip falls, the teeth are exposed, the upper lip is calm; on the count of two, the lower lip returns to its original position.
I.p. also. The lower teeth touch the upper lip and lightly stroke it, then the upper teeth make the same movement, touching the lower lip.
I.p. also. At the expense of "one" to collect the lips in a "piglet"; at the expense of "two" "piglet" moves to the right; at the expense of "three" - forward; at the expense of "four" - to the left.
I.p. also. Collect the lips in a “patch”, make circular movements clockwise and in the opposite direction.
I.p. - lips tightly closed, lower jaw slightly lowered. Under a strong stream of exhaled air, the lips part and the mouth opens wide.
3. Language exercises
We start by performing static exercises “tongue behind teeth, mouth open”, “scapula”, “cup”, etc. Next, we proceed to perform exercises to develop dynamic articulation (exercises are performed 4-5 times).
I.p. - the mouth is open, the tongue lies flat, the tip of the tongue is at the lower front incisors. At the expense of "one" with a sharp tip of the tongue, touch the inside of the left cheek, at the expense of "two" - the inside of the right cheek. The lower jaw is immobile.
I.p. - the mouth is open, the tip of the tongue is pressed against the inside of the lower teeth. With a push from the root, the tongue with its middle part should close with the alveoli of the upper teeth, while maintaining the position of the tip of the tongue, from which a click is formed.
I.p. - lips smile, the tip of the tongue is between loosely clenched teeth. With effort we push the tongue through the teeth, trying to move it as far as possible, and pull it back.
Section 3. Development of spatial representations.
SYNTHESIS OF FINGER GYMNASTICS
WITH ARTICULATION EXERCISES
Articulatory gymnastics is carried out simultaneously with the movements of the first hand of one hand, then both hands, imitating the movements of the jaw and tongue.
Since exercises of this type, in which the movement of the articulatory apparatus and the hands (first one, then both at the same time) are organically combined, are not described anywhere, it is on these exercises that the attention of teachers is focused in the manual.
lower jaw training
Exercise 1.1
A necessary condition for clear, good speech is the ability to open the mouth correctly. This is due to the work of the lower jaw.
Starting position: the head is held straight, the chin is in the usual comfortable position, the lips are closed.
At the expense of “one”, the jaw drops to a distance of the width of two fingers (middle and index), the tongue lies freely, the tip is at the lower incisors, the lips retain a rounded shape, the teeth are not exposed. When training, you need to ensure that the head does not tilt, all attention should be focused on lowering the jaw. At the expense of "two" we fix the open position of the mouth; at the expense of "three" the mouth is closed (the account is kept to oneself). Showing with the hand: 4 closed fingers, palm down, thumb pressed to the index finger. When the mouth opens, the thumb goes down, 4 fingers go up.
2. Training of the labial muscles
Exercise 2.1
Starting position: teeth are closed, lips in the usual calm state.
At the expense of “one”, the lips are pulled forward, as if taking the form of a “patch”; at the expense of “two”, the lips are stretched to the sides, without exposing the teeth (you should not stretch your lips especially strongly to the sides - you need to train them more in moving forward). The exercise is repeated three or four times without a break. Hand - all fingers are collected in a pinch, on "two" - fingers apart.
Exercise 2.2
At the expense of "one" lips are going to "piglet"; on the count of “two”, the “piglet” moves to the right, on the count of “three”, the collected lips move forward again, on the count of “four”, the “piglet” moves to the left, and then all movements in the same sequence are repeated three to four times. Hand - all fingers are collected in a pinch, the movements are synchronous with the movements of the lips.
Exercise 2.3
Starting position: see exercise 1.
At the expense of “one”, collect the lips in a “patch”, and then, trying not to unclench the “patch”, make circular movements; right, down, left, up. Repeat this circle three or four times, then do this exercise the same number of times from left to right. Hand - all fingers are collected in a pinch, the movements are synchronous with the movements of the lips.
Exercise 2.4
The lower teeth touch the upper lip and lightly scratch it, then the upper teeth make the same movement, touching the lower lip. The hand is motionless, palm up, only the fingers move. Palm down, only fingers move.
3. Tongue muscle training
Exercise 3.1
Starting position: the mouth is open, the tongue lies flat at the lower incisors.
At the expense of "one" the tongue rises behind the upper teeth, at the expense of "two" the tongue drops to its original position (the tongue is at the lower incisors). The exercise is repeated four to six times. Hand - palm movements up, down.
Exercise 3.2
Starting position: see exercise 1.
On the count of "one", touch the inside of the left cheek with the sharp tip of the tongue; at the expense of "two" - the inside of the right cheek. These movements are repeated three or four times without interruption; in this case, it is necessary to ensure that the lower jaw does not move. Hand - only the index finger moves, the rest of the fingers are gathered into a fist.
Exercise 3.3
Starting position: see exercise 1.
On the count of "one", stick out the tongue so as to feel the tension in the frenulum, then return it to its original position. Repeat the exercise three or four times. Hand - fingers are gathered into a fist. When the tongue protrudes, the fingers are straightened, tense, the palm is parallel to the table.
Exercise 3.4
Starting position: the mouth is slightly open, the lips smile, the tip of the tongue clicks, the jaw does not move, the tip of the tongue does not tuck. Hand - large and ring fingers clicks are made along with the tongue.
Exercise 3.5
This exercise is given to train the velum of the palate and the root of the tongue. The lips are closed, the tongue lies flat, the tip is at the lower front teeth. Without opening the lips and inhaling through the nose, lower the lower jaw to the deepest position with closed lips. There is a tense state of the muscles of the palatine curtain and the root of the tongue. Hold this state for a while, and then release the tension. Hand - palm down parallel to the table. When the lower jaw drops, the fingers gather into "binoculars".
With dysarthria, the motor mechanism of speech is disturbed due to an organic lesion of the central nervous system. The structure of the speech defect is a violation of the sound-producing side of speech.
Dysarthria is characterized by: violations of articulatory motility in the form of changes in the tone of the articulatory muscles, limitation of the volume of their voluntary movements, coordination disorders, various kinds of synkinesis, tremor, hyperkinesis of the tongue, lips; respiratory disorders; voice disorders.
Speech with dysarthria is slurred, fuzzy. The pace of speech is often disturbed, which can be accelerated (tachyllalia) or (more often) slow (bradilalia). Sometimes there are alternations of accelerated and slow tempo of speech. The phrase is formulated indistinctly, does not speak out, semantic stresses are randomly placed, the arrangement of pauses is disturbed, omissions of sounds, words, mumbling towards the end of the phrase are characteristic. There are also violations of the voice: the voice is usually quiet, often uneven - sometimes quiet, sometimes loud, monotonous, sometimes nasal, often hoarse. With dysarthria, violations of the lexical and grammatical side of speech are not leading. However, damage to the motor mechanisms of speech in the pre-speech period, combined with sensory disorders, can lead to complex disintegration and pathology of all parts of the speech development of a child with cerebral palsy.
In children with cerebral palsy, dysarthria is often combined with hearing loss, often there is an underdevelopment of phonemic hearing.
The classification of dysarthria is based on the principle of localization, the syndromological approach. In addition, the degree of intelligibility of speech to others is taken into account.
Based on the principle of localization, pseudobulbar, bulbar, extrapyramidal, cerebellar, cortical forms of dysarthria are distinguished.
Based on the syndromological approach, spastic-paretic, spastic-rigid, hyperkinetic and atactic forms of dysarthria are distinguished.
Observations show that classification according to the principle of localization is more appropriate due to the greater diagnostic clarity of various forms of dysarthria. In addition, a systematic approach to their analysis makes it possible to conduct speech therapy work more differentiated. Syndromic assessment of the nature of articulatory motility disorders is a significant diagnostic difficulty for a neuropathologist. It cannot be performed by a speech therapist, since it is based on a subtle differentiation of neurological syndromes. In addition, cerebral palsy is characterized by a change in neurological syndromes under the influence of therapy and evolutionary dynamics of development. Therefore, the classification of dysarthria according to the syndromological principle can also present certain difficulties.
In some cases it is useful to combine both approaches.
The classification of dysarthria according to the degree of understanding of speech for others was proposed by the French neurologist Tardieu (1968). They singled out four degrees of severity of speech disorders in children with cerebral palsy: 1) sound pronunciation disorders are detected only by a specialist in the process of examining a child; 2) violations of pronunciation are noticeable to everyone, but speech is understandable to others; 3) speech is understandable only to relatives of the child; 4) speech is absent or incomprehensible even to the relatives of the child. The fourth degree of violation of sound pronunciation, in essence, is an anarthria. Anarthria is understood as the complete or almost complete absence of sound pronunciation as a result of a violation of the motor innervation.
ions of the speech muscles. According to the severity of the manifestations of anartria, it can also be different: 1) the complete absence of speech and voice; 2) the presence of only voice reactions; 3) the presence of sound-syllabic activity.
Disorders of articulatory motility
1. Violations of muscle tone in the articulatory muscles. In all forms of dysarthria, there is a change in the muscle tone of the speech muscles. Changes in muscle tone in cerebral palsy have a complex pathogenesis. The nature of the violation of muscle tone in the articulatory muscles depends both on the localization of the lesion and on the characteristics of the disintegration of the entire reflex development. Therefore, in individual articulatory muscles, the tone can change in different ways and depend on the general posture of the child and the position of his head.
The following forms of violation of muscle tone in the articulatory muscles are distinguished.
1) Spasticity of the articulatory muscles. There is a constant increase in tone in the muscles of the tongue, sometimes lips. The tongue is tense, drawn back, its back is spastically curved, raised upwards, the tip of the tongue is not pronounced. The tense back of the tongue raised to the hard palate will help soften consonant sounds. A feature of articulation with spasticity of the muscles of the tongue is palatalization. Since palatalization has an independent phonemic meaning in Russian, this articulation disorder can cause phonemic underdevelopment. So, pronouncing the same words like ardor and dust, they say and moth, the child may not differentiate their meaning.
An increase in muscle tone in the circular muscle of the mouth leads to spastic tension of the lips, tight closure of the mouth. Active movements with spasticity of the articulatory muscles are limited. So, the inability to move the tongue forward may be associated with a sharp spasticity of the geniolingual, maxillohyoid and digastric muscles, as well as the muscles attached to the hyoid bone.
Spasticity of the articulatory muscles is often combined with an increase in muscle tone in the muscles of the face and neck, as well as general spasticity of the skeletal muscles.
One of the most powerful cervical muscles is the sternocleidomastoid. These muscles in children with cerebral palsy may be spastically tense on one or both sides. Unilateral tension of the sternocleidomastoid muscle is usually observed due to the severity of the asymmetric cervical tonic reflex (ASTR). The spastic tension of these muscles can determine or increase the incorrect position of the child's head, prevent its active movements, and the sufficient development of clavicular breathing. The muscles of the floor of the mouth and the root of the tongue are directly connected with the cervical muscles. The tension of the muscles of the neck further limits the mobility of these muscles, as well as the movements of the lower jaw.
Spasticity of the articulatory muscles and cervical muscles can be enhanced by the influence of the cervical tonic and labyrinth tonic reflexes. In these cases, the relaxation of the muscles of the articulatory apparatus must begin with the choice of such special postures in which tonic reflexes either do not appear at all, or are minimally manifested. With severe spasticity, classes begin in the following reflex inhibiting positions:
1. Reflex inhibiting position 1. It is used when the labyrinth tonic reflex is pronounced. In the supine position, the head, shoulders and neck of the child are somewhat bent; the back, hips and knees are also bent. Muscle relaxation is achieved by uniform smooth swings.
2. Reflex inhibiting position 2. It is used when the neck-tonic reflex is pronounced. In the position on the back, the legs are slightly bent at the knee joints, the arms are extended along the body. The speech therapist places his hand under the child's neck, allowing the head to lean back freely, while the shoulders are somewhat bent, the neck is extended.
3. Reflex forbidding position 3. It is also used for the severity of the cervical tonic reflex. The position on the back with legs and arms extended and the head slightly thrown back.
After an adequate posture is chosen to reduce the influence of postural reflexes, they begin to relax the muscles of the neck, face, and articulatory apparatus using special techniques.
The next step is to relax the neck muscles. Here are some examples of exercises.
Exercise 1. The child lies on his back in the inhibition position 2, the head hangs back a little, one hand of the speech therapist is on the back of the child’s neck, with the other hand he makes rhythmic movements of the child’s head of a circular nature, first clockwise, then counterclockwise. Several passive movements are made, then the child is stimulated to perform active movements.
Exercise 2. The child is in the same position. But his head hangs slightly over the edge of the table. At the same time, it is placed on a swinging board. In this position, the same rhythmic circular movements of the head are made. At first, these movements are made passively, then passively-actively. Finally, the child makes active movements. They are easier to perform under a score or a musical melody.
Exercise 3 Child in prone position. The head hangs over the edge of the table. The same movements are made.
The next stage of work is relaxation of the muscles of the face. With severe spasticity, this relaxation is performed in the reflex of the final position 1.
First of all, a relaxing massage of the facial muscles is performed. The massage starts from the middle of the forehead towards the temples. The massage is performed at a slow pace. Musical accompaniment (slow, smooth rhythm) contributes to relaxation. Massage should make the child feel good. In some children with cerebral palsy, hypersensitivity of the entire facial and especially articulatory areas may be noted. A simple tactile touch can make them feel uncomfortable and increase muscle tone. Therefore, a relaxing facial massage should not be applied immediately to all areas of the face.
The second direction of relaxing facial muscle massage is the movement from the eyebrows to the scalp. Movements are made with both hands evenly on both sides.
The third direction of massaging hands is to move down from the line of the forehead, cheeks to the muscles of the neck and shoulders.
Relaxation of the labial muscles in severe spasticity is carried out in a reflex of the inhibiting position 2. The speech therapist places his index fingers on a point located between the middle of the upper lip and the corner of the mouth on both sides. The direction of movement of the fingers to the middle of the lips. In this case, the upper lip is collected in a vertical fold. The same movement is made in relation to the lower lip, and then to both lips.
During the next exercise, the index fingers of the speech therapist are placed in the same position, but the movement goes up on the upper lip, exposing the upper gums, and down on the lower lip, exposing the lower gums.
During the next exercise, the speech therapist places the tips of his index fingers in the corners of the child's mouth, stretches the child's lips with his fingers. With a reverse movement, the lips return to their original position.
These exercises are carried out with a different position of the mouth: the mouth is closed, ajar, half-open, wide open.
After relaxing the lips, their passive-active movements are trained. The child is taught to drink through a straw, to grab and hold candies and sticks of various sizes with his lips. To conduct such exercises, a speech therapist must have a set of sterile sticks. The speech therapist should preheat them and place them in sweet syrup.
These exercises help to normalize the position of the mouth. It has already been noted that in the spastic state of the muscles of the lips, the mouth is tightly compressed. Its arbitrary opening in this case is difficult. Sometimes, with a spastic condition of the upper lip, the mouth may, on the contrary, be open; at the same time salivation is usually sharply expressed. The lack of control over the position of the mouth greatly complicates the development of voluntary articulatory movements. Therefore, after some relaxation of the facial and labial muscles has been achieved, the child's mouth, which is in the reflex forbidding position, is passively given a normal position. The child sees the position of the mouth in the mirror. The speech therapist fixes the child's attention on the feeling of a closed mouth. Then the normalization of the position of the mouth is passive-actively carried out at different positions of the child. Observations show that in severe forms of cerebral palsy, in some cases, the child closes his mouth more easily with a slightly bent head and more easily opens it voluntarily with his head slightly tilted back. Initially, these lightweight techniques are used. The easiest reflex inhibiting position for closing the mouth is often the position of the child on the side with bent legs and slightly lowered head. In the same position, the child is taught to actively open the mouth. The child lies on its side with its mouth closed. The speech therapist places his index fingers on the upper lip and a point located between the middle of the upper lip and the corner of the mouth, and thumbs at the same points on the lower lip and makes a slight pushing movement (the upper lip rises up, the lower lip goes down together with the lower jaw). Movements are made in a small volume. Thus, the speech therapist achieves a narrow opening of the mouth. Then the same exercises are performed by the child in positions (poses) that are more difficult for him. The transition from passive to active mouth-opening movements is often made possible through reflex yawning.
After these preparatory exercises, active voluntary movements are trained according to verbal instructions. At the initial stages, pictures are used for this. Here are some of these instructions: "Open your mouth wide", "Pull your lips forward", "Lips in a calm state", "Collect the lips with wrinkles and return them to their original relaxed position."
Tasks are offered to imitate the position of the mouth shown in the pictures. Gradually, the exercises become somewhat more complicated: the child is asked to blow through relaxed lips, to produce vibrational movements.
Spastic tension in children with cerebral palsy is usually most pronounced in the muscles of the tongue. Therefore, you should never start relaxing with the muscles of the tongue. You need to start with the exercises above. Work on relaxation of the muscles of the tongue always begins after general muscle relaxation. After general relaxation, the next task is to relax the entire tongue. It should be taken into account that the own muscles of the tongue (during the contraction of which the movements of the entire tongue occur) are closely connected with the muscles of the lower jaw. Therefore, the movement down in the oral cavity of the spastically raised tongue and thus its relaxation is most easily achieved with the simultaneous lowering of the lower jaw (opening the mouth). For school-age children, such exercises are offered in the form of auto-training: “You are calm, completely relaxed, your tongue lies calmly in your mouth. Slowly lower it down as the lower jaw drops."
If these techniques are not enough, then it is considered useful to put a piece of sterile gauze or a sterile stopper on the tip of the tongue. The resulting tactile sensation helps the child to understand that something is interfering with the free movements of the tongue, i.e. feel a sense of spasticity. After that, the speech therapist uses a spatula or tongue depressor to apply light horizontal pressure to relax the tongue.
The next relaxation technique is light, smooth swaying movements of the tongue to the sides. The speech therapist very carefully grabs the tongue with a piece of sterile gauze and smoothly rhythmically moves it to the sides.
In addition, acupressure is used to relax the muscles of the root of the tongue. For acupressure, the so-called "action points" are used, which are characterized by increased electrical conductivity. These points are found using a portable tobiscope diagnostic device. These points are detected by a speech therapist and a doctor during a special joint examination of the child. In some cases, these points are located under both angles of the lower jaw. Having placed fingers on these points, the speech therapist makes rotational movements with the pad of the thumb, index or middle finger. At first, these movements are superficial; then (after 0.5-1 min) they are performed with great pressure; after this they move on to surface movements. These points are massaged daily for 1.5-2 minutes.
An important technique for relaxing the muscles of the tongue is its passive-active movements. These relaxing movements are best done when the baby is lying on his stomach. The speech therapist takes the tongue of the child in his hand through a sterile bandage. Then it produces pendulum swings of the tongue (“hanging swing”). Gradually, the passive help of a speech therapist decreases. The child begins to perform these exercises more and more actively.
Relaxation of the muscles of the tongue contributes to the normalization of articulation, and in particular the elimination of palatalization.
2) Disturbances in the tone of the articulatory muscles can also manifest themselves in the form of hypotension. With hypotension, the tongue is thin, flattened in the oral cavity, the lips are flaccid, they cannot close tightly. Because of this, the mouth is usually half open, hypersalivation is pronounced.
Nosalization can be a feature of articulation in hypotension. In this case, the hypotension of the muscles of the soft palate prevents sufficient movement of the palatine curtain upward and its pressing against the posterior wall of the pharynx. A stream of air exits through the nose. The jet of air coming out through the mouth is extremely weak. In addition, with hypotension, the pronunciation of labial-labial stop noisy consonants is disturbed. p", p, b", b. With hypotension, palatalization is difficult. In this regard, the pronunciation of deaf stop consonants is especially disturbed. In addition, when a bow is formed at the moment of pronouncing deaf consonants, more energetic work of both lips is necessary.
More easily with hypotension, labial-labial occlusive nasal sonants are pronounced - mm", as well as labio-dental fricative noisy consonants (f, f", v, v"), the articulation of which requires loose closure of the lower lip with the upper teeth and the formation of a flat gap. However, the sounds c, f can be pronounced without their characteristic velarization. This is due to the fact that with hypotension it is often not possible to lift the back of the back of the tongue to the soft palate. In addition, these sounds may have a nasal connotation.
With hypotension, the pronunciation of the anterior lingual stop noisy consonants is also disturbed. t, t", d, d". In addition, the articulation of the anterior lingual fricative monofocal consonants is distorted. s, s", s, s", as well as anterior lingual fricative bifocal consonants w, w. Often there are various types of sigmatism. Interdental and lateral sigmatism are especially common. There are other articulation disorders.
In case of hypotension of the muscles of the articulatory apparatus, a firming massage is used (more intense stroking movements, elements of forceps-like stroking of the labial and chewing muscles, etc.). Of particular importance in hypotension is articulatory gymnastics using resistance.
3) Violations of the tone of the articulatory muscles in cerebral palsy can also manifest themselves in the form dystonia(changing character of muscle tone). At rest, low muscle tone may be noted, while trying to speak, the tone increases sharply. Dystonia sharply and in many ways distorts articulation. Moreover, a characteristic feature of these disorders is their dynamism, inconstancy of distortions, substitutions and skipping of sounds.
An assessment of the state of the tone of the articulatory muscles should be carried out by a speech therapist together with a neuropathologist.
II. The next characteristic sign of impaired articulatory motility in dysarthria is impaired mobility of the articulatory muscles.
Limited mobility of the articulatory muscles is the main manifestation of paresis or paralysis of these muscles. This is what determines the structure of the defect in dysarthria.
Insufficient mobility of the articulatory muscles causes a violation of sound pronunciation. With damage to the muscles of the lips, the pronunciation of both vowels and consonants suffers. Among vowels, the pronunciation of labialized sounds is especially disturbed, the pronunciation of which is associated with the specific work of the lips. These are the sounds OU; when they are pronounced, active movements of the lips are required: rounding, stretching forward. Among consonants, the pronunciation of labial occlusive sounds is primarily violated (n, p", b, b", m, m"). The child cannot stretch the lips forward, round them, stretch the corners of the mouth to the sides, lift the upper lip up and lower the lower lip down, and perform a number of other movements. Insufficient lip mobility often disrupts articulation as a whole, as these movements change the size and shape of the vestibule of the mouth, thereby affecting the resonance of the entire oral cavity.
Sound pronunciation is especially grossly disturbed with a sharp restriction of the mobility of the muscles of the tongue. In this case, there may be an insufficiency of lifting the tip of the tongue up in the oral cavity. This is usually associated with a violation of the innervation of the stylohyoid, digastric, hyoid-pharyngeal, maxillofacial, lingual-pharyngeal, stylolingual and lingual-palatine muscles. In these cases, the pronunciation of most sounds suffers, requiring both raising the tip of the tongue up and the combined work of these muscles ( l, r, f, w, c, h, d, t and some others).
In violation of the innervation of the clavicular-hyoid, thyroid-hyoid, maxillo-hyoid, chin-lingual and digastric muscles, the ability of the tongue to move down is limited. This can adversely affect the pronunciation of hissing and whistling sounds, front vowels (and, uh) and some other sounds.
In violation of the innervation of the hyoid-pharyngeal, scapular-hyoid, awl-hyoid, digastric (posterior abdomen) and some other muscles, the ability of the tongue to move backward is limited. This disrupts the articulation of posterior lingual sounds. (g, k, x), as well as some vowels, especially mid and low (uh oh ah)
With paresis of the muscles of the tongue, it is often impossible to change its configuration, push it forward, pull it back, make various lateral movements, etc. All this disrupts the sound pronunciation of most sounds.
Sound pronunciation is even more disturbed due to the limited mobility of the muscles of the soft palate (palato-pharyngeal, palatoglossal and a number of other muscles). With damage to the muscles of the soft palate, the voice acquires a nasal tone.
With dysarthria, paresis of the muscles of the facial muscles is often noted, which also negatively affects sound pronunciation. So, paresis of the temporal muscles, chewing muscles limit the movements of the lower jaw. Spasticity and paresis of the cervical muscles also adversely affect articulation.
The limited mobility of the articulatory muscles in dysarthria determines the need to use special gymnastics in speech therapy work. When conducting articulatory gymnastics, as well as while working on general motor skills, tactile-proprioceptive stimulation, the development of static-dynamic sensations, and clear articulatory kinesthesia are of great importance. At the initial stages, work is carried out with the maximum connection of intact analyzers (visual, auditory, tactile). The tactile analyzer plays a large role in kinesthetic perception. Therefore, before articulatory gymnastics, a massage of the articulatory muscles is performed. The nature of the massage depends on the characteristics of the violation of muscle tone. At subsequent stages of work, for the development of more clear and differentiated articulatory kinesthesia, the participation of other intact analyzers is gradually excluded. Many exercises the child is asked to perform with their eyes closed. At the same time, his attention is focused on proprioceptive sensations. Articulatory gymnastics is differentiated depending on the form of dysarthria and the severity of the lesion of the articulatory apparatus.
Before working on the speech muscles, exercises are carried out in order to develop the facial muscles of the face. Already in preschool children, they are trying to develop the ability to voluntarily perform differentiated facial movements and exercise control over them. The child is taught to close and open his eyes, frown, puff out his cheeks. During the development of facial muscles, the child is taught to voluntarily swallow saliva, close and open the mouth. If the child does not have a developed chewing function, the speech therapist gives him a bun or biscuit and teaches him to chew in front of a mirror. These exercises are combined with special classes during which the child is taught to voluntarily close and open the mouth.
To develop sufficient tension and strength of the muscles of the face and lips, special exercises are used. To do this, use special sterile wipes, tubes. The child covers the tube or napkin with his lips and tries to hold it, despite the speech therapist's attempts to pull it out of his mouth. For the development of the muscles of the lips, special exercises are offered to stretch the lips forward with a tube, stretch them to the sides, by alternating these movements.
Articulatory gymnastics of the muscles of the tongue begins with the cultivation of an active touch with the end of the tongue to the edge of the lower teeth. Then general, less differentiated tongue movements are developed. At first, this development takes place in a passive, and then in a passive-active plan. Finally, the child performs these movements in an active way. These exercises begin by moving the tongue forward and retracting it back into the mouth. In some children with cerebral palsy, the tongue moves forward during suckling. This is due to the fact that in a healthy child of the first months of life, the movements of the tongue are closely related to the sucking reflex. Reflex development disorders, which, as we have seen, are an essential mechanism of motor and speech disorders in children with cerebral palsy, can manifest themselves in the long-term preservation of the sucking reflex and, in connection with this, in the participation of this reflex in the forward movement of the tongue. The task of the speech therapist is to suppress the sucking reflex and the simultaneous development of voluntary movements of the tongue.
Stimulation of the muscles of the root of the tongue begins with their reflex contractions. The speech therapist achieves a reflex contraction of these muscles by pressing with a spatula on the root of the tongue. These movements are fixed with the help of unconditioned reflex, and then voluntary coughing movements.
An important section of articulatory gymnastics is the development of more subtle and differentiated movements of the tongue. Initially, these movements are performed in a passive, and then passive-active plan. Finally, the voluntary execution of these movements is achieved. One of the tasks of such differentiated articulatory gymnastics is to delimit the movements of the tongue from the movements of the lower jaw. For this, exercises to stimulate the movements of the tip of the tongue with an open mouth and a fixed lower jaw can be useful. used series special exercises to activate the rise of the tip of the tongue.
Play therapy is widely used in the development of articulatory motor skills. Games are selected depending on the nature and severity of the damage to articulatory motor skills, as well as taking into account the age of the child. With some adaptation, games published in the literature can be used.
Work on the development of articulatory motor skills is effective only when it is combined with the general complex treatment of the child, with the development of his general motor skills and manual skills. Simultaneously with the work of a speech therapist, a methodologist in physical therapy develops supporting, grasping, manipulative activities of the hands and fine differentiated finger movements. At the same time, the methodologist brings up clear finger kinesthesia and prepares the hand for writing. The teacher stimulates the manipulative activity of the hands and forms various manual skills. So, for example, children are taught to knead and roll plasticine, squeeze rubber pears with their hands, grab small objects with their fingertips, fold mosaics, draw, sculpt, cut, hatch, color pictures, fasten and unfasten buttons, hooks, lace up shoes, use a spoon and fork , correctly hold a pencil, a pen.
When conducting classes, the speech therapist must monitor the posture of the child. Before classes, he achieves relaxation of the muscles of the hands by shaking them and stroking the massage. In this case, the possibility of the influence of pathological postural reflexes is always taken into account. The speech therapist makes sure that the child's head, legs and arms are in the correct position. The child's hands should be on the table in a relaxed state, the palm and fingers are pressed to the table. When conducting articulatory gymnastics, accompanying movements in the fingers are suppressed.
Respiratory disorders
Breathing problems almost always occur with dysarthria in children with cerebral palsy. They have a complex pathogenesis associated with paresis of the respiratory muscles, changes in their tone, impaired reciprocal coordination, and delayed maturation of the respiratory functional system. The latter is manifested in the fact that many children with cerebral palsy, even at school age, may be dominated by "infantile" breathing patterns. These schemes are usually combined with general violation reflex development, with the severity of pathological postural reflexes. Therefore, the normalization of breathing in children with cerebral palsy is closely related to the general pathogenetic task of therapy - the normalization of reflex development.
Schematically distinguish vegetative and speech respiration. Speech breathing is closely related to voice formation. For the normal functioning of the vocal apparatus, a certain correspondence is necessary between the tension of the inhaling and exhaling muscles. These muscles are antagonists. The inspiratory muscles increase the volume of the chest during inhalation; exhaling muscles - reduce its size and volume. The former include: the anterior serratus muscle, as well as the external intercostal muscles. The diaphragm is a powerful inspiratory muscle. The pectoralis major, pectoralis minor, and external intercostal muscles are also of great importance for speech breathing.
For the production of active speech exhalation, fine coordinated work of all respiratory muscles is required: tension of the muscles that carry out inhalation is necessary, all except for the diaphragm, which, although it participates in inhalation, relaxes at the moment of exhalation and gradually moves upward, i.e. functions in conjunction with the expiratory muscles. If at the moment of exhalation the diaphragm, together with other muscles that carry out inhalation, is tense, speech exhalation will be sharply disturbed.
An important role in the violation of active exhalation in children with cerebral palsy is played by the general insufficient volume of breathing, which is due to their low physical activity.
Respiratory disorders in children with cerebral palsy are due to the insufficiency of the central regulation of respiration, as well as the pathology of the motor functional system. Respiratory function improves significantly after birth as the child's central nervous system develops. In the first months of life, the child is dominated by the abdominal type of breathing, breathing is shallow, frequent. The respiratory rate of one minute gradually decreases with age. According to A. Peiper, the respiratory rate per minute is up to 1 month - 22-72 respiratory movements; from 1 to 6 months - 21-58; from 6 months to 2 years - 25-45; from 2 to 5 years - 21-40; from 5 to 10 years - 15-31. After 6 months, the abdominal type of breathing is replaced by a mixed one, the chest is more and more actively included in the respiratory movements, breathing becomes deeper and less frequent. Thus, diaphragmatic breathing is phylogenetically older than chest breathing.
As already noted, children with cerebral palsy are characterized by infantile breathing patterns: the predominance of abdominal breathing, its high frequency and insufficient depth. In addition, disturbances in the rhythm of breathing are characteristic: at the time of speech, breathing quickens, after pronouncing sounds, the child often makes superficial convulsive breaths. Often there are violations of coordination between breathing, phonation and articulation. In all cases, active exhalation is impaired, which is shortened and usually occurs through the nose, despite the constantly half-open mouth. The severity of respiratory disorders usually corresponds to the severity of the general motor impairment. Respiratory disorders are especially pronounced in the hyperkinetic form of cerebral palsy.
In children with hyperkinetic form of cerebral palsy, sometimes there was a violation of the scheme of respiratory movements due to spasmodic contractions of the abdominal muscles and mismatch in the work of the muscles that carry out inhalation and the muscles that carry out exhalation. Such disturbances were aggravated by incorrect movements of the diaphragm, its spasmodic tension at the moment of active speech exhalation. This led to the fact that the child had a tendency to speak not on exhalation, as is the case in the norm, but on inspiration. Hyperkinesis of the respiratory muscles made it difficult, and sometimes impossible, to voluntarily control respiratory movements. Respiratory disorders sharply increased due to the severity of pathological postural reflexes. Therefore, with the severity of these reflexes, breathing exercises must be carried out in reflex inhibiting positions,
Breathwork begins with general breathing exercises. The purpose of these exercises is to increase the volume of breathing and normalize its rhythm. Here are some of these exercises.
Exercise 1. The child lies on his back. The speech therapist bends his legs at the knee joints and with bent legs presses on the armpits. These movements are performed in a normal respiratory rhythm by counting: "one" - bending the legs, "two" - pressing them on the armpits, "three" - returning the legs to their original position. This exercise helps to normalize the movements of the diaphragm.
Exercise 2. The child sits with his mouth closed. Then one nostril is blocked. The child breathes to a certain rhythm (account or click of a metronome). Then the second nostril is clamped to the child. The same cycle of breathing movements is repeated.
Exercise 3. The child is sitting. A "fan of air" is created in front of his nostrils. Under the influence of this air, the depth of inspiration increases.
Simultaneously with general breathing exercises, it is very important to teach children with cerebral palsy how to blow their nose correctly. Mastering this skill contributes to the formation of an extended voluntary exhalation. To consolidate this function, it is necessary to rely on sensations as much as possible. The child must "see" and hear his exhalation. For this purpose, it is recommended to use various respirators, it is recommended to blow through a pipette, tube or straw into a jar of carbonated water. The child blows into a straw and watches as bubbles appear. Then blows with eyes closed to enhance kinesthetic sensations. At subsequent stages, the child is given instructions: “Make big bubbles, look, listen”, “Make small bubbles, look, listen”, “Do alternately: one small, one big bubble”, “Make small bubbles to a certain rhythm or count”. These exercises allow you to differentiate nasal exhalation (when blowing your nose) from oral exhalation (during blowing) and make oral exhalation as voluntary and rhythmic as possible, as well as long enough.
Then the child is taught to voluntarily combine and feel inhalation through the nose after exhalation through the mouth (the child makes small bubbles). A variety of techniques are used to "specify" the oral exhalation. Ping-pong balls or inflatable balls are placed on the table. The child is asked to blow so that the ball (or ball) spins on the table or falls to the floor. The oral exhalation is supported by the sensations of air on the hand. First, a speech therapist blows on the child’s hand, drawing his attention to the feeling of air: “You feel the air, you feel the wind.” Then the child himself blows on his hand.
There are also special exercises for training nasal exhalation. The child is instructed not to open his mouth. In some cases, the speech therapist keeps the child's mouth closed. The child is given the instruction: "Inhale deeply and exhale for a long time through the nose." After a while, the child begins to follow the position of his mouth. Exercises with a respirator help to voluntarily control nasal exhalation. The child takes a deep breath through the nose. The speech therapist places the tip of the respirator in the right and then in the left nostril of the child. The child is blowing. Small bubbles appear in the respirator can, and then (according to the instructions) large bubbles. Then the same exercises are performed using a handkerchief. The child takes a deep breath through the nose, exhales alternately through the right, then the left nostril. When exhaling, one nostril is clamped with a handkerchief. When carrying out such exercises, be sure to monitor the posture of the child, the position of his arms, legs, head, back. Let's call the basic rules of breathing exercises. You can not overwork the child. It is necessary to ensure that he does not strain his shoulders, neck and does not take the wrong posture. The child's attention should be focused on the sensations from the movements of the diaphragm, intercostal muscles and muscles of the lower abdomen. The child should make all respiratory movements smoothly, under the account or under music. Breathing exercises should be carried out before meals, in a well-ventilated area.
Let's give examples of speech breathing exercises.
a) The speech therapist closes the child's nostrils and asks him to inhale through his mouth until he asks him to pronounce individual vowel sounds or syllables.
b) The child is asked to inhale through the mouth. The speech therapist puts his hands on the child's chest, as if preventing inhalation for 1-2 seconds. This contributes to a deeper and faster inhalation and a longer exhalation.
c) The child is asked to hold the breath as long as possible, thus achieving a slower and deeper breath, followed by a slow and prolonged exhalation.
Such exercises are recommended to be carried out daily for 5-10 minutes. During these exercises, at the moment the child exhales air, the speech therapist pronounces various vowel sounds. At the same time, he varies the volume and tone of the voice. Then he asks the child to imitate him. It is recommended to pronounce the following rows of vowels (in a whisper and loudly):
at ____ay ____wow ____ya ____; O ____OU ____ao ____oa ____;
uh ____yiu. ____and about____ ia ___; and ____eu. ____oo ____ea ____
Then the child is stimulated to pronounce fricative consonants in isolation and in combination with vowels:
f ____With ____w ____X ___; af ____ash, ____ace ____;
pho ____co ____sho ____.; F ___si ___syu _____;
F ___sa ___sha ___, as well as voiceless and voiced explosive consonants and other sounds.
In the process of practicing speech breathing, special exercises-games are of great importance: soap bubbles, blowing out candles, blowing small fluffs and papers off the table, etc. Games are selected differentially depending on the age and nature of the respiratory disorder. With various variations, those games that are described in speech therapy literature can be used. Work on breathing, phonation and articulation is carried out in close unity; special logarithmic exercises and games are of great importance in this work.
Classes in logorhythmics should be carried out both with children of preschool and school age. In these classes, exercises for the development of general and articulatory motor skills, breathing and voice are carried out with musical accompaniment. Many observations suggest that music promotes general and local muscle relaxation, reduction of violent movements, coordination and coordination of movements. Therefore, a whole range of movements that are inaccessible to the child in a normal environment can be performed by him to musical accompaniment.
Among the logarithmic exercises, there are: introductory, regulating muscle tone, activating attention, educating a sense of rhythm, specifically speech.
As an illustration, we present fragments of logarithmic lessons. These exercises can be done with both preschool and school age children.
Exercise 1. The development of the pace of movement. Instructions: "When slow music sounds, walk slowly in place", "When the music is fast, speed up your step to run." With severe motor disorders, children do these exercises while sitting. At the same time, it is important that children lean on the entire foot, keeping their heads in a straight position, and do not open their mouths during exercises.
Exercise 2. Sound development and voice development. Instruction: “After a musical loss, pronounce the syllables in chorus: sa, so, su, sy." The exercise is carried out at an accelerated pace.
A characteristic feature of dysarthria in children with cerebral palsy is voice impairment. Melody-intonation disorders are among the main and often the most persistent signs of dysarthria. It is they who have the greatest influence on the intelligibility, emotional expressiveness of children's speech. Voice disorders are caused by paresis of the muscles of the tongue, lips, soft palate, vocal folds, larynx muscles, changes in their muscle tone and limitation of mobility. In this case, paresis of the muscles of the larynx is of the greatest importance. In particular, this applies to the cricothyroid muscles, which stretch the true vocal cords. When the muscles of the larynx are affected, the voice becomes weak, non-melodious.
The antagonists of the muscles that stretch the vocal cords are the sternothyroid muscles, which, when contracted, lower the larynx, thereby reducing the tension of the true vocal cords. For normal voice formation, the coordinated work of these two muscle groups is necessary. In children with cerebral palsy, especially in its atonic-astatic and hyperkinetic forms, the coordinated work of these muscle groups is disrupted. This causes voice disorders.
The movements of the larynx are closely related to the movements of the tongue, palate, and lower jaw. Therefore, with severe spasticity of these muscles and a sharp restriction of their movements, pronounced voice disorders are usually observed.
The vibration of the vocal cords is of great importance for the production of voice. Spasmodic contraction of the muscles of the vocal apparatus can disrupt the possibility of vibration of the vocal cords, which will impede the formation of voiced consonants. Voiced consonants in these conditions will be replaced by deaf ones.
Insufficiency of proprioceptive impulses from the organs of articulation of breathing and voice formation in all cases aggravates voice disorders in children with cerebral palsy.
Voice disorders in children with cerebral palsy are extremely diverse. At various forms dysarthria they are specific. However, the most often noted are insufficient voice power (the voice is weak, quiet, dries up during speech), deviations in the timbre of the voice (deaf, nosalized, hoarse, monotonous, choked, dull; it can be guttural, forced, tense, intermittent, etc.) , weak expression or absence of voice modulations (the child cannot arbitrarily change the pitch). It should be emphasized that voice disorders in children with cerebral palsy are significantly enhanced when their postural reflexes are pronounced. Therefore, in these cases, work on the voice should begin in reflex prohibitive positions. Work on the voice is always only one of the links in the complex rehabilitation of children with cerebral palsy. For the development of the voice in these children, various orthophonic exercises contained in speech therapy literature can be used. The purpose of these exercises is to develop the coordinated activity of breathing, articulation and phonation. In children with cerebral palsy, these exercises are modified depending on the form of dysarthria and the clinical picture of the disease in general. So, in children with cerebral palsy at the initial stages of work on the voice, in some cases, a positive effect can be achieved by using the so-called "chewing method" proposed by E. Frechels. According to this method, the child is asked to pronounce the first sounds available to him at the time of chewing.
Work on the voice always begins with general relaxation, articulatory massage and articulatory gymnastics. For children with cerebral palsy, it is especially important to relax the muscles of the neck at the time of pronouncing sounds, as well as the chain of vowels and - uh- O - at- a- s.
A large place in speech therapy work is occupied by circular movements of the head, activation of the movements of the soft palate: swallowing drops of water, coughing, yawning, pronouncing a vowel sound a on a hard attack. Exercise is carried out in front of a mirror, counting. The speech therapist draws the child's attention to the sensation of the palatine curtain being raised and held in this position (account). The following exercises can be used as preparatory exercises:
a) stimulation of the back of the tongue and palate with light patting movements using a tongue depressor;
b) teaching voluntary swallowing. A speech therapist from an eyedropper drips a drop of water against the back wall of the pharynx. The head of the child is somewhat thrown back;
c) stimulation of cough-like movements and yawning.
Normal voice formation is possible if the child can open and close his mouth, lower his lower jaw, and imitate chewing movements. A speech therapist can stimulate the lifting of the lower jaw by lightly and rhythmically tapping the child's chin (jaw trembling reflex). After some time, the child masters the ability to independently raise the lower jaw. After that, he is taught the ability to lower the lower jaw. Initially, the lower jaw of the child is lowered by the speech therapist (by 1.0-1.5 cm). Then the speech therapist asks the child to do it on their own. Gradually, the child's jaw drops to the optimal distance. During these exercises, it is advisable to use a model that is a brightly colored ball tied to a rope. At the moment of lowering the lower jaw, the child pulls the ball down. Then he can perform this exercise with his eyes closed, visualizing the ball dropping down. During the exercises, voluntary control over the volume and pace of movement is trained.
As control over movement develops, visual stimulation using facial expressions gradually ceases. The child is instructed to lower the lower jaw and at the same time pronounce various combinations of sounds, for example: “Lower the lower jaw as low as possible and at the same time imitate the cry of a crow: “kar-kar”, “Exaggerate the movements of the jaw when pronouncing vowels”, etc.
To strengthen the muscles of the palatine curtain, exercises are used in alternating its relaxation and tension. For example, the child is asked to make a sound before the end of the yawning movement. a and with the mouth wide open, go from pronouncing this sound to the sound and, holding air in the mouth under pressure before making an explosive sound and, to draw the attention of the child to the sensation of the state of the palatine curtain. To strengthen the muscles of the palatine curtain, the child is asked to alternately pronounce the following sounds:
n-pa-m-pa; m-buy-m-buy etc.
In addition to organically conditioned voice disorders, various functional stratifications can be observed, primarily due to the general emotional state of the child. It is well known that when excited children with cerebral palsy tend to fall into whispers and silent speech. Therefore, in the process of verbal communication in children with cerebral palsy, it is very important to create an emotionally positive background (“a situation of confidence”). When working on the voice, it is very useful to use as much singing and expressive recitation as possible together with the speech therapist. Of great importance is the slow pronunciation of vowels. Sounds are pronounced alternately - sometimes in a whisper, then loudly.
At the same time, they are working on increasing the length of the speech exhalation: at first, two vowels are pronounced on one exhalation (a-uh; o-u; u-s; uh etc.), then three ( a-uh-oh; oh-oh-and etc.) and finally four (ah-ah-ah-ah and etc.). Then syllables are pronounced with a gradual lengthening of their chains, then - words with certain sounds, at the last stages - poems, tongue twisters; the latter are pronounced with a change of stress and an acceleration of the tempo of speech, sometimes in a whisper, sometimes loudly.
Exercises to develop strength, timbre and voice pitch are important. One example of such exercises can be counting in tens (ten, twenty, thirty, etc.) with a gradual strengthening (direct counting) and with a weakening (reverse counting) of the voice, as well as pronouncing letters in alphabetical order, reading poems with a gradual strengthening and weakening of the voice. For the development of the pitch and timbre of the voice, various speech therapy games, reading fairy tales by roles, dramatizations, etc. are of great importance. Dramatization games played by children also help develop the melodic-intonation side of speech, flexibility and modulation of the voice. When selecting speech material, it is necessary to take into account the following factors: the structure of the defect, age, intelligence, a specific speech therapy task, as well as the education of the moral and ethical aspects of the individual. When working with preschoolers, poems by K.I. Chukovsky "Telephone", "Fly-clatter", poems by S.Ya. Marshak, A.L. Barto, S.V. Mikhalkov. When working with school-age children, it is useful to use the fables of I.A. Krylov, poems by A.S. Pushkin, N.A. Nekrasov, V.V. Mayakovsky and our other excellent poets and prose writers.
Dysarthria in children with cerebral palsy manifests itself in the form of two groups of symptoms: negative, associated with a delay in the formation of certain levels of the speech functional system, and pseudo-positive, due to the presence of early reflex automatisms. Examples of negative symptoms can be: underdevelopment of the intonational side of speech, insufficiency of voluntary articulatory movements, underdevelopment of the lexico-grammatical and semantic side of speech, as well as phonemic analysis, etc. Pseudopositive symptoms are manifested in the presence of congenital unconditioned reflex activity, uncharacteristic for children of this age. Therefore, this activity is pathological. Examples of pseudo-positive symptoms can be the persistence of reflexes of oral automatism for a number of years, the presence of primitive infantile patterns of breathing, swallowing, biting, chewing, etc. Negative symptoms are overcome in the process of overcoming the underdevelopment of the function, pseudo-positive ones should be inhibited and suppressed. Such a dual symptomological approach to the manifestations of cerebral palsy is widely reflected in both domestic and foreign literature. Our long-term clinical and pedagogical research has shown the feasibility of such an approach to overcoming speech disorders in children with cerebral palsy. The development of speech function in children with cerebral palsy is closely related to the active suppression of pseudo-positive symptoms. Only in children of the very first months of life, at the initial stages of work, such innate unconditioned reflexes as sucking, swallowing, reflex oral and other movements are stimulated in order to develop the synaptic pathways necessary for the formation of arbitrary articulatory and swallowing movements.
At the subsequent stages of work, these reflexes are actively suppressed and replaced by more advanced forms of motor activity. As you know, the same evolutionary principle is the basis of stimulation motor development in children with cerebral palsy. For example, the development of voluntary movements is preceded by inhibition of postural reflexes. Below is a description of the reflexes that prevent the development of voluntary motor activity of the articulatory apparatus.
1. Sucking reflex. With tactile irritation of the lips, the anterior surface of the tongue and the hard palate, sucking movements occur. The reflex changes after 4 months and goes out by the end of the year.
2. Lip reflex. When patting on one of the corners of a slightly half-open mouth, an involuntary movement of the lips occurs, closing the mouth is a preparation for sucking. After 6 weeks, the reflex gradually fades away.
3. Swallowing reflex. Occurs under the influence of tactile stimulation of the back of the tongue, palate, posterior pharyngeal wall. Swallowing usually follows sucking activity. In the neonatal period, swallowing precedes the sucking reflex. The change in the pattern of swallowing and sucking begins at 12 weeks.
4. Proboscis reflex. Patting in the area of the middle of the upper lip causes a reflex movement of the lips forward, they are pulled into the "proboscis" - a reflex of preparation for sucking. Fades away after 6 weeks.
5. Search reflex. Irritation of the cheek in the area of the corner of the mouth causes the lips to move towards the stimulus - a reflex of preparation for sucking. Fades away after 6 weeks.
6. Palmar-roto-head reflex. It is caused by pressure on the palm in the area of the eminence of the thumb. At the same time, the mouth opens, the head bends. The reflex fades after 6 weeks.
7. Mouth opening reflex. Occurs at 4 months. It is caused by visual stimulation - at the sight of a breast or a bottle of milk, the child reflexively opens his mouth (conditioned associative reflex, begins to fade from 6 months).
8. Emotional communicative reflexes of laughter and smiling (laughter appears from 16 weeks, smile from 4-6 weeks). After 6 months, they are converted into arbitrary differentiated reactions.
9. Biting reflex. When a stimulus is placed between the gums, the mouth closes and the stimulus is retained. The reflex disappears by 4 months.
10. Unconditioned reflex oral movements. They are caused by tactile irritation of some main facial points. So, light blows in the area of the corner of the mouth cause the lowering of the corresponding half of the lower lip. Tactile irritation of the cheek from the corner of the mouth towards the lower lip causes the head and tongue to move towards the stimulus. Tactile stimulation of the middle of the upper or lower lip causes the lip and tongue to rise or fall, tactile stimulation of the chin in the up or down direction causes extension (when moving up) and flexion (when moving down) of the head and opening the mouth.
Dysarthria in children with cerebral palsy is complicated by the presence of many of these reflexes. Therefore, one of the important tasks of correctional work is the suppression of these reflexes. For this purpose, the child is given an appropriate reflex forbidding position. The speech therapist gently touches the child's lips with a cotton swab, with the other hand preventing the reflex movement of the lips. Other reflexes are extinguished in the same way. It is important to carry out these exercises systematically, 2-3 times a day. For students, these exercises should be a special kind of speech therapy homework.
A feature of dysarthria in children with cerebral palsy is not only the insufficiency of voluntary articulatory movements, but also the weakness of their kinesthetic sensations. Therefore, during speech therapy work, it is necessary to be guided by the principle of motor-kinesthetic stimulation.
During exercises for the development of articulatory motor skills, the child's attention is always drawn to the sensations that arise (we are talking about kinesthetic sensations). For the development of motor-kinesthetic feedback, it is important to perform the following exercises daily: shaking the upper and lower lips, straightening the cheeks (lifting them from the dental arch), lowering and raising the lower jaw, placing the tongue under the lower and upper incisors, lightly patting the palatine curtain. At first, the child sees these movements in the mirror in front of him. Then the mirror is removed. Finally, during these exercises, sit with your eyes closed. In this case, the kinesthetic sensations that arise during exercise are enhanced.
In addition, it is necessary to train the following articulatory-sensory schemes daily:
a) Double circuit. The upper and lower lips are passively closed, held in this position. Attention is fixed on the feeling of closed lips. The child is then asked to blow through the lips.
b) Labio-dental scheme. With the index finger of the left hand, the speech therapist lifts the child's upper lip, exposing his teeth. With the index finger of the right hand, the speech therapist raises the child's lower lip to the level of the upper incisors. At the same time, he asks the child to blow.
c) Lingual-alveolar scheme. The speech therapist presses and holds the tip of the child's tongue against the alveolar process. The child is asked to blow.
d) Glosso-palatine scheme. The child's head is somewhat retracted, the back of the tongue rises to the hard palate. The child is asked to make coughing movements, fixing attention on the sensations of contact between the tongue and palate and the cessation of this contact.
An important section of speech therapy work with dysarthria are exercises for the development of articulatory praxis. Articulatory praxis is formed in the process of speech experience on the basis of clear kinesthetic sensations and the development of voluntary coordinated movements of the articulatory system. For the development of articulatory praxis in children with cerebral palsy, early speech therapy work, the expansion and enrichment of the child's speech experience, as well as the predominance of special syllabic exercises over purely articulatory ones are of great importance. Special series of syllables are selected, the pronunciation of which involves a successive change of various articulatory movements.
Exercises in pronouncing syllables in the initial stages should be carried out at a slow pace. At the same time, it is necessary to fix the child's attention on the motor sensations that arise in him. Here are some of these syllable exercises: be-ve-ba-va-za-da-zha-ra-ha; wa-ba; ba-va; base; ba-da; lady; bar-ra; ba-ha; wa-ba; for-ba; yes-ba; toad; ra-ba; ha-ba and etc.
The most difficult section of speech therapy work for dysarthria is work on pronunciation. All the sections described above constitute, as it were, its preparatory stage. Work on pronunciation is strictly differentiated depending on the form of dysarthria, the age of the child, the state of his intellect, the level of speech development, etc. However, it is necessary to take into account some general principles of this work. We will review these principles below.
1. The speech therapist must remember that his main task is the development of speech communication, and not teaching the correct pronunciation of sounds. Therefore, work on sound pronunciation should always facilitate (rather than impede) verbal communication and improve the social adaptation of the child.
2. From the point of view of the general characteristics of the disease, the child should always be assessed in a comprehensive manner, taking into account his motor and mental development, and the general prognosis of the disease. These data must be compared with the characteristics of the social environment. Depending on this comparison, the criteria for assessing the severity of sound pronunciation disorders may be different. So, the same severity of sound pronunciation disorders in a child in a social security institution can be assessed as mild, based on the characteristics of his needs and environment, and the same severity of violations in a student of a special school can be assessed as severe, since they can significantly impede learning and school adaptation in general.
3. An important aspect of the work is the formation of motives that encourage the child to overcome violations of sound pronunciation.
4. A speech therapist needs to develop a differentiated sound analysis in a child.
5. Great importance is attached to strengthening the perception of articulatory structures based on visual-kinesthetic sensations.
6. Work on individual sounds should be consistent. You should start with those sounds, the articulation of which in this child is more preserved. For example, if a child, by imitation, pronounces a sound correctly, then they start with this sound. Or they choose those sounds that can be pronounced correctly in certain words or contexts. Sometimes sounds are selected according to the principle of simpler motor coordination, but always taking into account the structure of the articulation defect. From the number of defective sounds, the sounds of early ontogenesis are selected first of all, i.e. those sounds that, during normal development, are the first in a child’s speech to be pronounced correctly.
7. A differentiated approach is used to the successive stages of work on the correction of incorrectly pronounced sounds. If the child's speech is not clear to others, it is advisable to start working with individual sounds or with sounds in syllables. If the child's speech is relatively understandable and in some words he can pronounce defective sounds correctly, the speech therapist works to correct the sounds in various words. Then the correct pronunciation is fixed in various contexts and speech situations.
8. It is necessary to take into account the influence of pathologically enhanced postural reflexes on sound pronunciation and prevent its negative consequences with the help of special exercises in reflex inhibiting positions.
The main methods of sound pronunciation correction are: motor-kinesthetic and auditory-visual-kinesthetic.
In preschool children, dysarthria is usually combined with a general underdevelopment of speech. In the process of work, it is important to correct the child as little as possible, especially not to interrupt his speech with the words: “Speak correctly”, “Repeat after me”, etc. Otherwise, speech negativism (up to the refusal of verbal communication) and stuttering may occur. It is more appropriate to use the techniques of play therapy in combination with individual work on articulation, phonation and breathing.
The effectiveness of speech therapy work on sound pronunciation largely depends on its correct assessment. Along with the use of the generally accepted methodology in speech therapy for examining speech for dysarthria in children with cerebral palsy, a speech therapist should pay attention to the following:
To note whether there is a correspondence between the severity of articulatory motor disorders and the severity of sound pronunciation disorders;
Conduct a detailed phonetic study and analyze phonetic disorders. For example, a child has a sound substitution v on the b. It is necessary to establish the reason for this replacement (most common cause is insufficient lip tension);
Assess the relative strength and persistence of phonetic disorders in various situations of speech communication;
Assess the ease with which incorrect pronunciation can be corrected;
The severity of the incorrect pronunciation of each sound should be assessed depending on its position in the word (initial, middle, final);
All violations of sound pronunciation should be assessed according to three main parameters: distortion, replacement, sound skip.
It is highly desirable to record the child's speech on a tape recorder at the beginning and at the end of the speech therapy course. When conducting an examination, a speech therapist must learn to listen at one time or another only one of the incorrectly pronounced sounds. It is necessary to carefully prepare speech material. The child should be given such tasks, in the performance of which he would be able to independently pronounce words with the sound being examined.
The overall severity of the speech impairment can be assessed using a rating scale from "1" to "5" for each sound in a different position. Rating "5" - the sound is normal, "4" - weak sound distortion, "3" - strong sound distortion, "2" - sound replacement, "1" - no sound.
It is useful to compare the data obtained with the overall assessment of the severity of the disease.
In all cases, it is important to determine the severity and persistence of sound pronunciation disorders. To do this, the speech therapist must observe the child's speech in the following speech situations.
1. The child speaks freely without being aware that he is being watched. The speech therapist enters into a casual conversation with the child on a topic of interest to him; game contact is established with preschool children. The speech therapist watches how the child pronounces sounds during a conversation with parents, comrades, answers at the blackboard, etc.
2. The child names the objects from the pictures. The speech therapist notes whether sound pronunciation improves due to the perception of pictures.
3. The child reads words and texts. It is noted whether reading improves sound pronunciation, in addition, the speech therapist fixes whether defective sound pronunciation affects the understanding of texts.
4. The child repeats a memorized series of words (for example, counting to ten, repeating the days of the week, months, seasons, short poems).
The data obtained during the survey are used to differentiate the methods of work. For example, if a child pronounces sounds better when naming objects from pictures, a speech therapist will rely more on visual stimuli. If the child pronounces sounds better in the memorized series of words, then the speech therapist will include more poetic speech in his classes, accompanying the pronunciation of syllables with their rhythmic tapping.
In addition, it is necessary to record whether the sound improves